

Metformin selectively inhibits metastatic colorectal cancer with the KRAS mutation by intracellular accumulation through silencing MATE1
- PMID: 32444490
- PMCID: PMC7293710
- DOI: 10.1073/pnas.1918845117
Metformin selectively inhibits metastatic colorectal cancer with the KRAS mutation by intracellular accumulation through silencing MATE1
Abstract
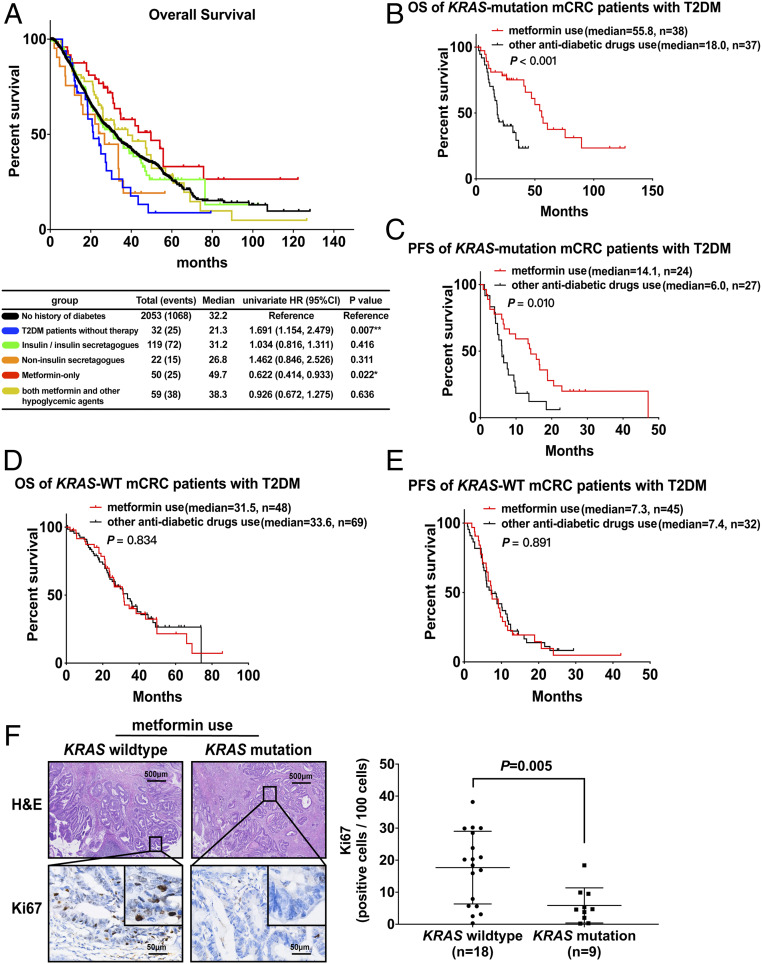
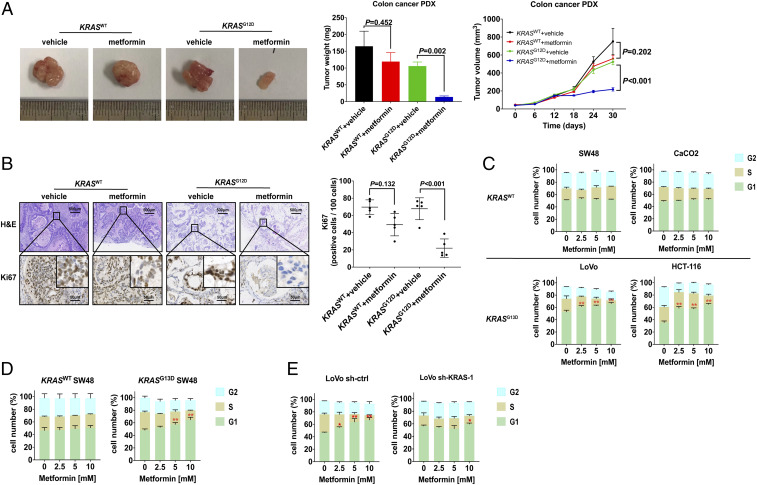
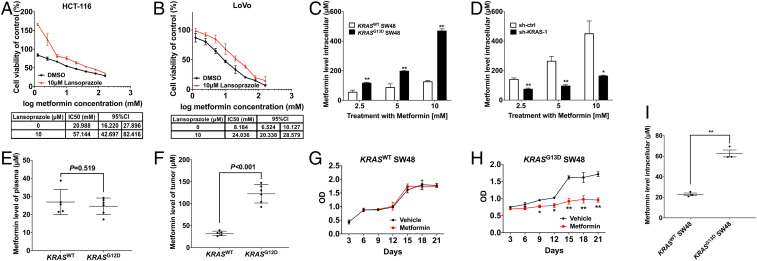
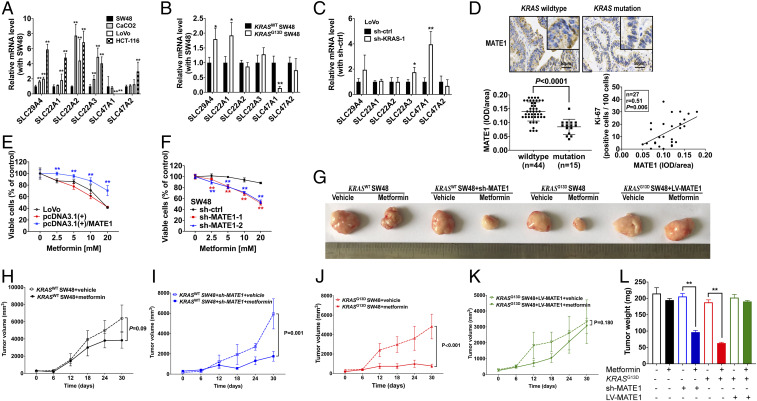
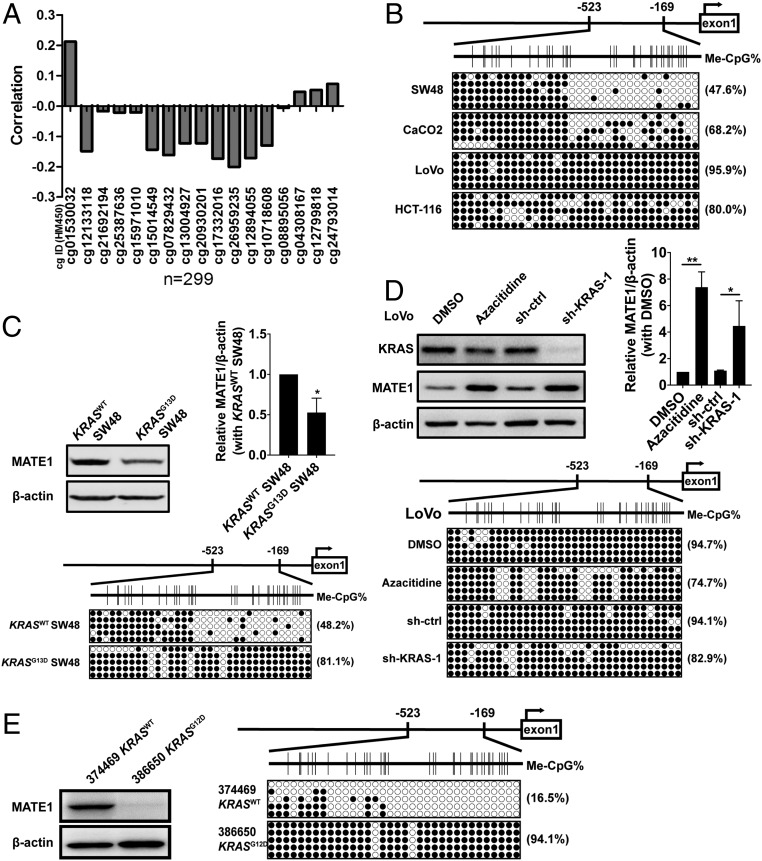
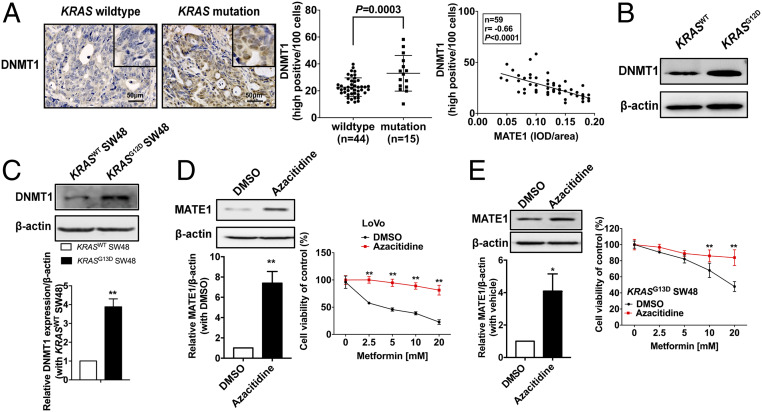
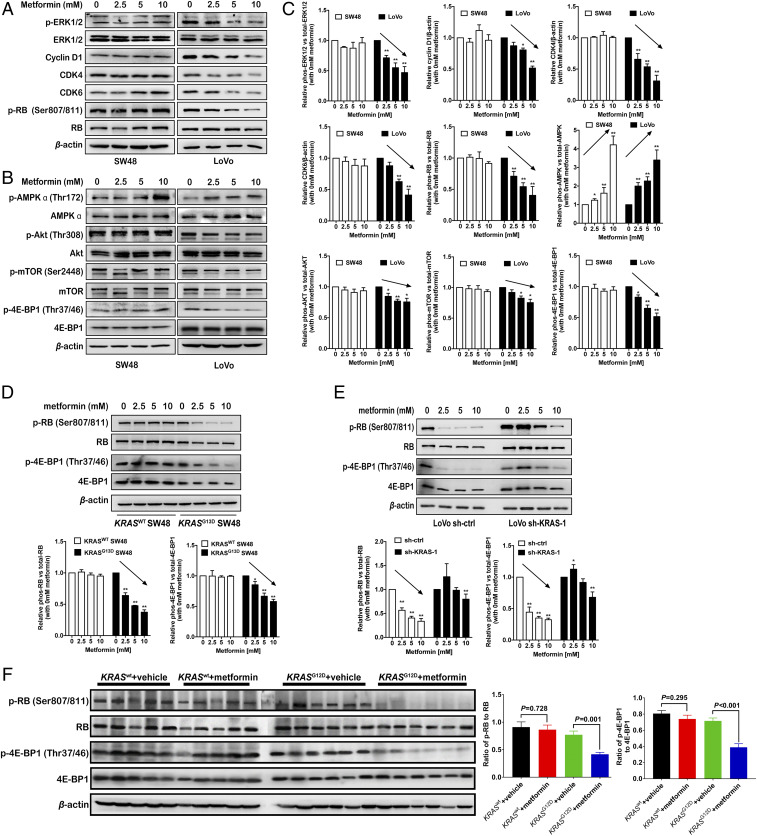
Metastatic colorectal cancer (mCRC) patients have poor overall survival despite using irinotecan- or oxaliplatin-based chemotherapy combined with anti-EGFR (epidermal growth factor receptor) drugs, especially those with the oncogene mutation of KRAS Metformin has been reported as a potentially novel antitumor agent in many experiments, but its therapeutic activity is discrepant and controversial so far. Inspiringly, the median survival time for KRAS-mutation mCRC patients with diabetes on metformin is 37.8 mo longer than those treated with other hypoglycemic drugs in combination with standard systemic therapy. In contrast, metformin could not improve the survival of mCRC patients with wild-type KRAS Interestingly, metformin is preferentially accumulated in KRAS-mutation mCRC cells, but not wild-type ones, in both primary cell cultures and patient-derived xenografts, which is in agreement with its tremendous effect in KRAS-mutation mCRC. Mechanistically, the mutated KRAS oncoprotein hypermethylates and silences the expression of multidrug and toxic compound extrusion 1 (MATE1), a specific pump that expels metformin from the tumor cells by up-regulating DNA methyltransferase 1 (DNMT1). Our findings provide evidence that KRAS-mutation mCRC patients benefit from metformin treatment and targeting MATE1 may provide a strategy to improve the anticancer response of metformin.
Keywords: DNA methyltransferase 1 (DNMT1); KRAS mutation; metastatic colorectal cancer; metformin; multidrug and toxic compound extrusion 1 (MATE1).
Copyright © 2020 the Author(s). Published by PNAS.
Conflict of interest statement
The authors declare no competing interest.
Figures
References
-
- Siegel R. L., Miller K. D., Jemal A., Cancer statistics, 2018. CA Cancer J. Clin. 68, 7–30 (2018). - PubMed
-
- Cremolini C. et al., FOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as first-line treatment of patients with metastatic colorectal cancer: Updated overall survival and molecular subgroup analyses of the open-label, phase 3 TRIBE study. Lancet Oncol. 16, 1306–1315 (2015). - PubMed
-
- Allegra C. J. et al., Extended RAS gene mutation testing in metastatic colorectal carcinoma to predict response to anti-epidermal growth factor receptor monoclonal antibody therapy: American Society of Clinical Oncology Provisional Clinical Opinion update 2015. J. Clin. Oncol. 34, 179–185 (2016). - PubMed
-
- Douillard J. Y. et al., Panitumumab-FOLFOX4 treatment and RAS mutations in colorectal cancer. N. Engl. J. Med. 369, 1023–1034 (2013). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
