

Comprehensive review of evaluation and management of cardiac paragangliomas
- PMID: 32444502
- PMCID: PMC7482425
- DOI: 10.1136/heartjnl-2020-316540
Comprehensive review of evaluation and management of cardiac paragangliomas
Abstract
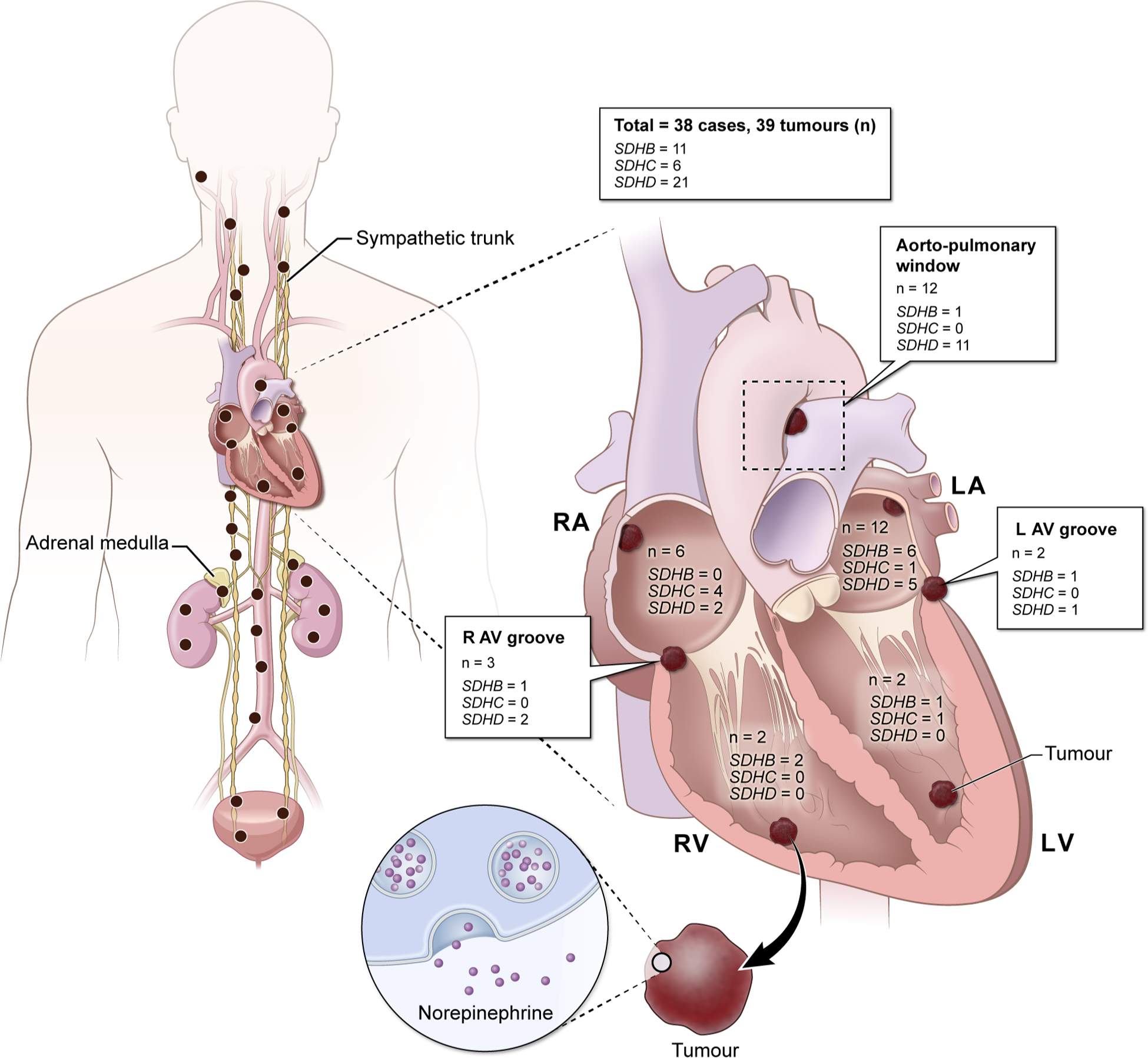
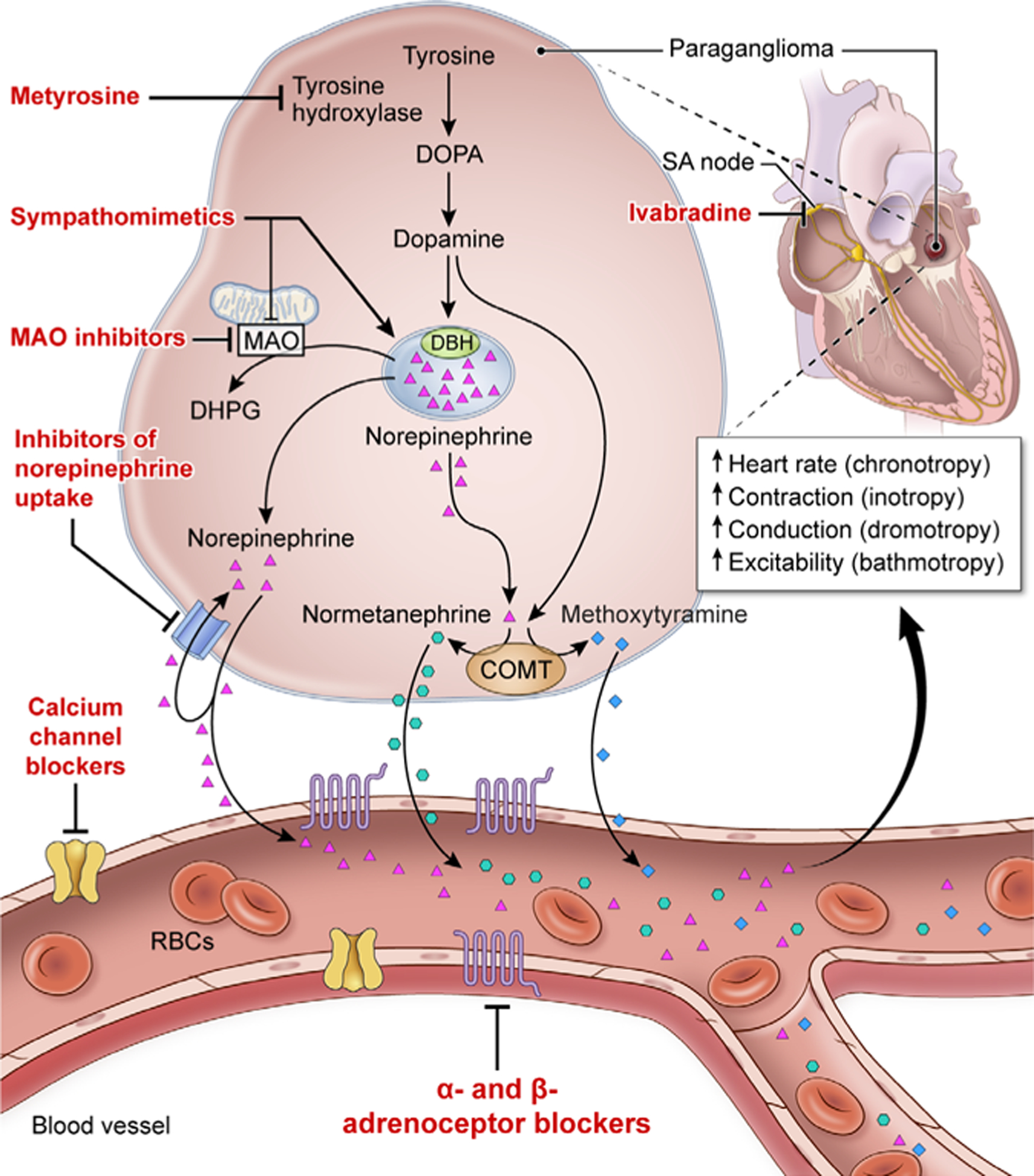
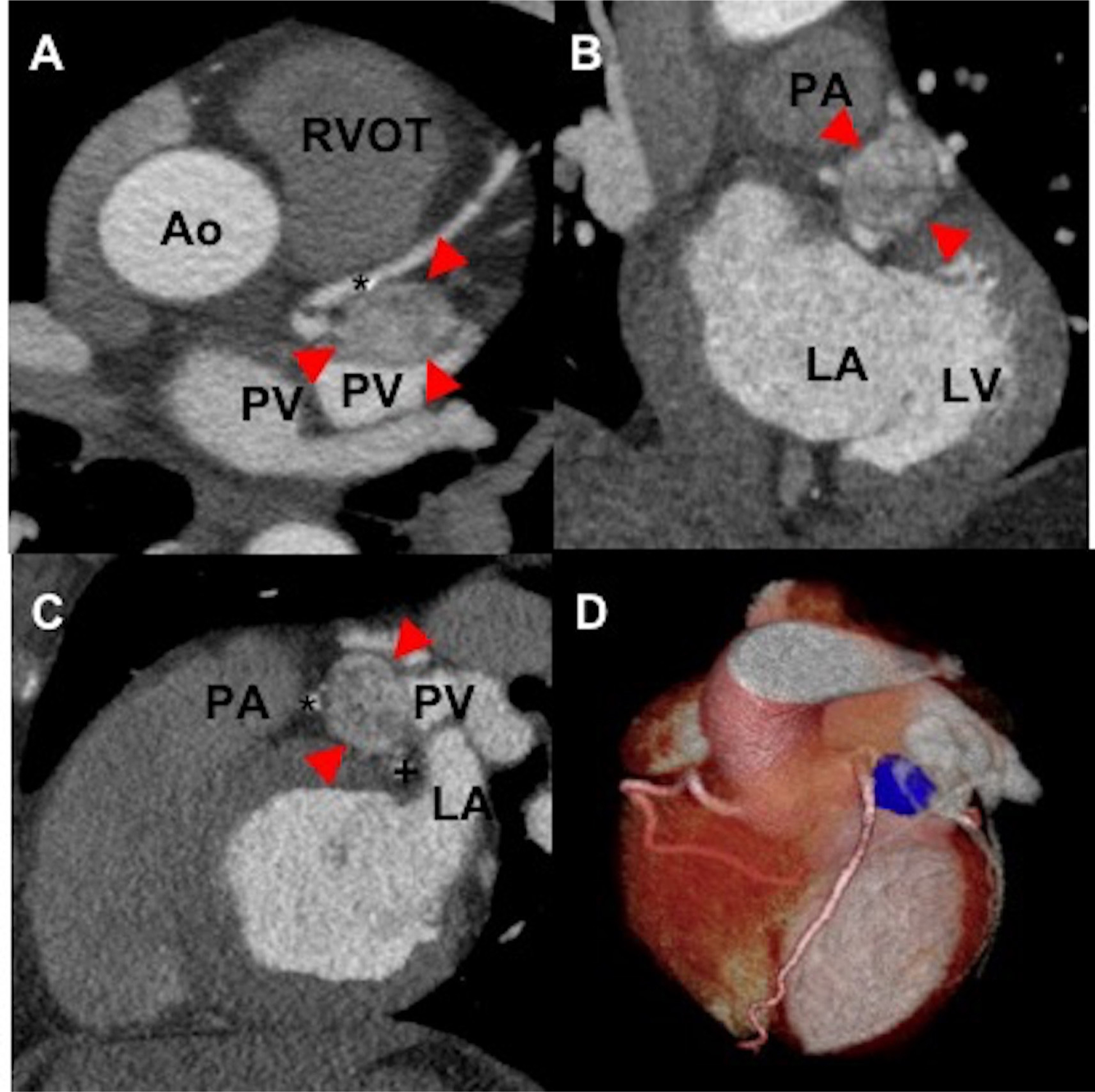
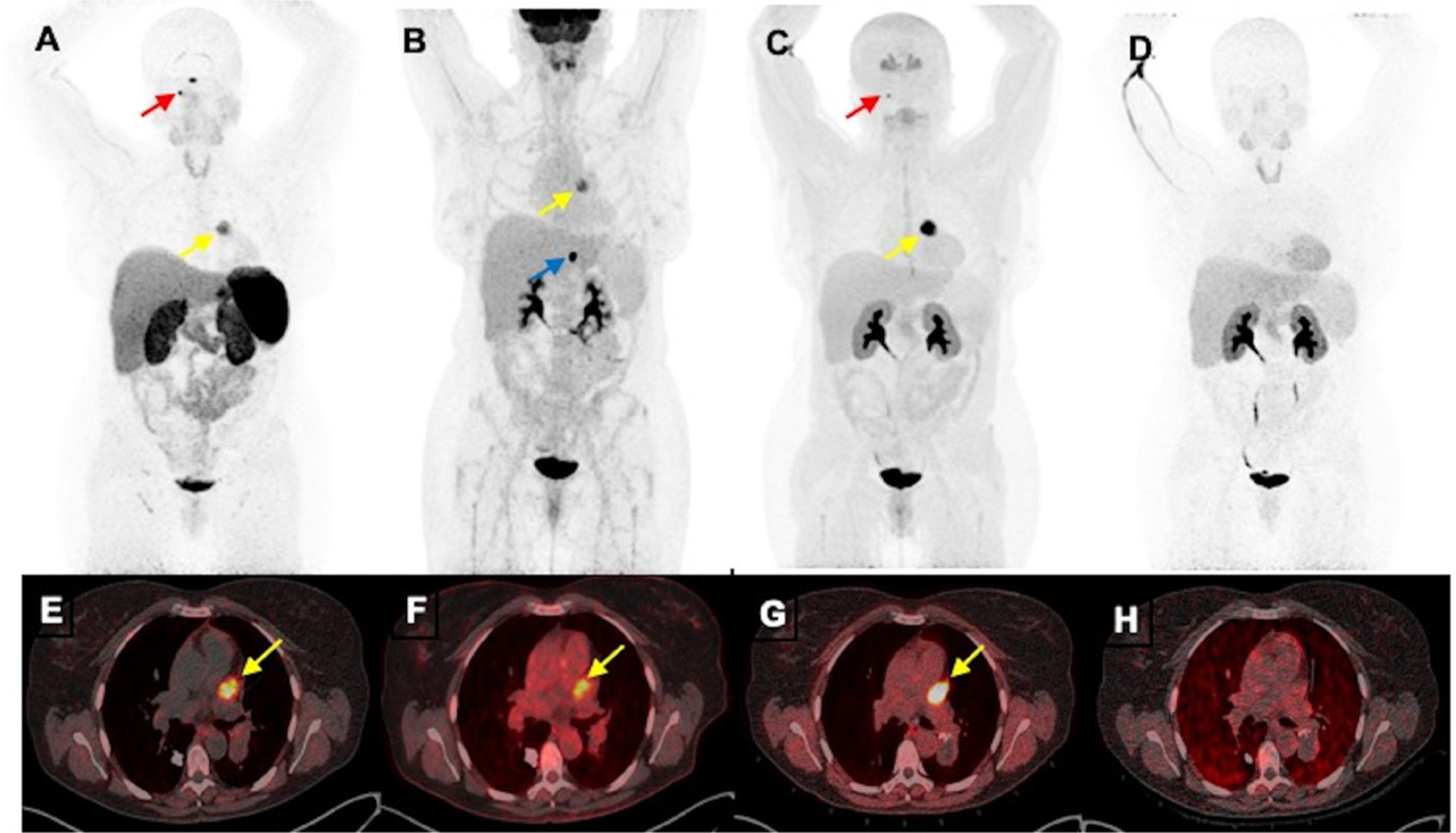
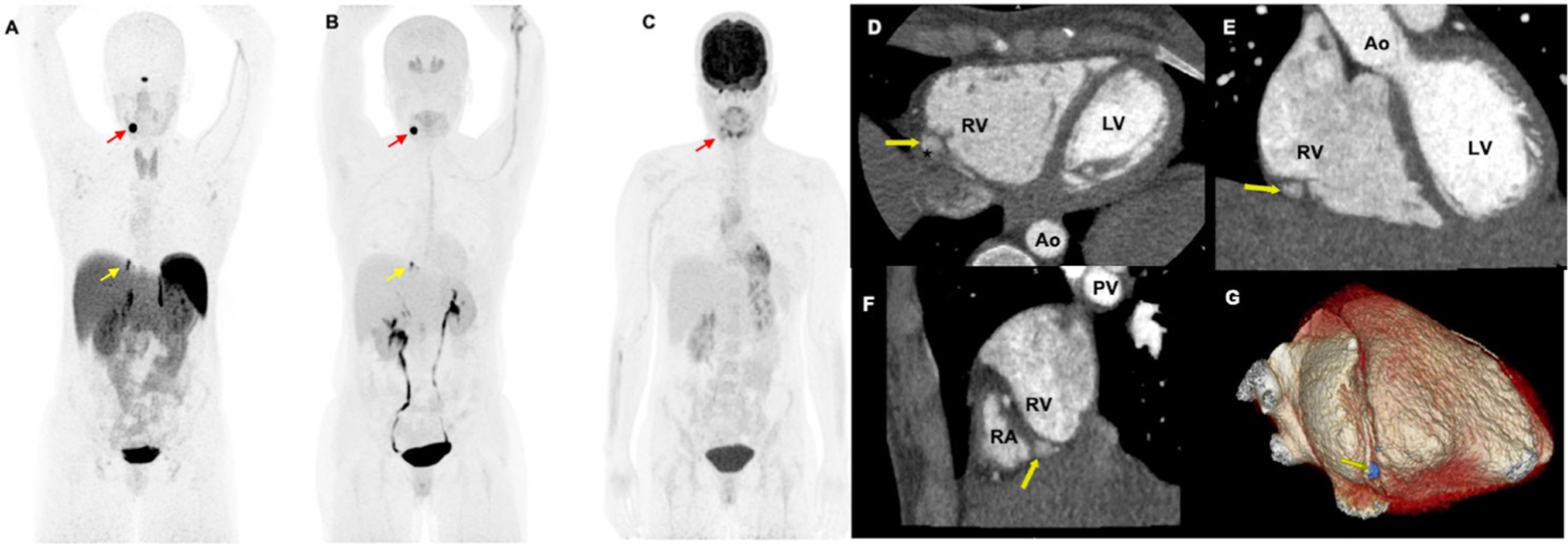
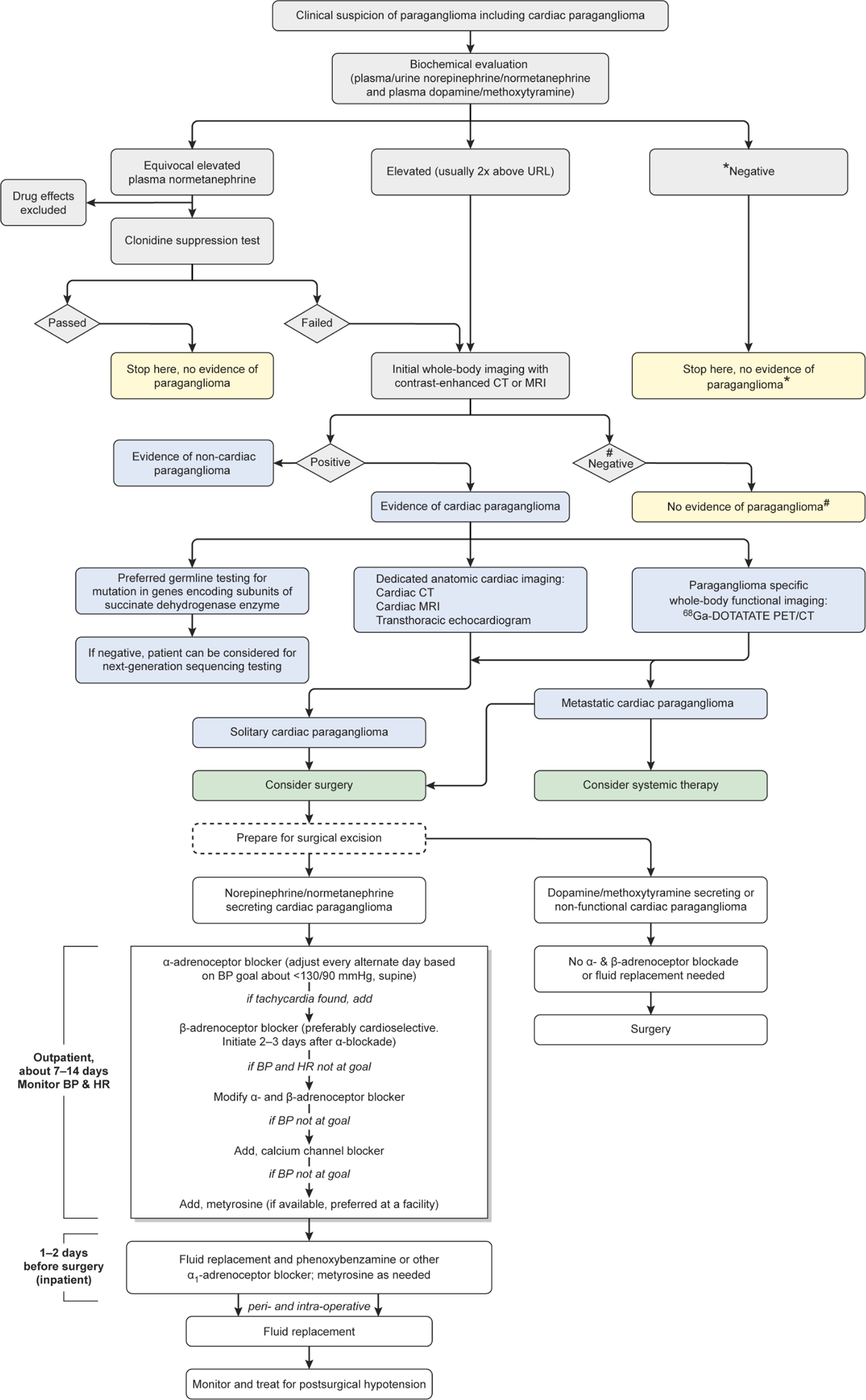
Cardiac paraganglioma (PGL) is a rare neuroendocrine tumour causing significant morbidity primarily due to norepinephrine secretion potentially causing severe hypertension, palpitations, lethal tachyarrhythmias, stroke and syncope. Cardiologists are faced with two clinical scenarios. The first is the elevated norepinephrine, whose actions must be properly counteracted by adrenoceptor blockade to avoid catastrophic consequences. The second is to evaluate the precise location of a cardiac PGL and its spread since compression of cardiovascular structures may result in ischaemia, angina, non-noradrenergic-induced arrhythmia, cardiac dysfunction or failure. Thus, appropriate assessment of elevated norepinephrine by its metabolite normetanephrine is a gold biochemical standard at present. Furthermore, dedicated cardiac CT, MRI and transthoracic echocardiogram are necessary for the precise anatomic information of cardiac PGL. Moreover, a cardiologist needs to be aware of advanced functional imaging using 68Ga-DOTA(0)-Tyr(3)-octreotide positron emission tomography/CT, which offers the best cardiac PGL-specific diagnostic accuracy and helps to stage and rule out metastasis, determining the next therapeutic strategies. Patients should also undergo genetic testing, especially for mutations in genes encoding succinate dehydrogenase enzyme subunits that are most commonly present as a genetic cause of these tumours. Curative surgical resection after appropriate α-adrenoceptor and β-adrenoceptor blockade in norepinephrine-secreting tumours is the primary therapeutic strategy. Therefore, appropriate and up-to-date knowledge about early diagnosis and management of cardiac PGLs is paramount for optimal outcomes in patients where a cardiologist is an essential team member of a multidisciplinary team in its management.
Keywords: cardiac CT imaging; cardiac imaging and diagnostics; genetics; positron emission tomographic (PET) imaging; systemic review.
© Author(s) (or their employer(s)) 2020. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Lam AK-Y, Lam AK. Update on adrenal tumours in 2017 World Health organization (who) of endocrine tumours. Endocr Pathol 2017;28:213–27. - PubMed
-
- Patel J, Sheppard MN. Pathological study of primary cardiac and pericardial tumours in a specialist UK centre: surgical and autopsy series. Cardiovasc Pathol 2010;19:343–52. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous