

Physical multimorbidity, health service use, and catastrophic health expenditure by socioeconomic groups in China: an analysis of population-based panel data
- PMID: 32446349
- PMCID: PMC7241981
- DOI: 10.1016/S2214-109X(20)30127-3
Physical multimorbidity, health service use, and catastrophic health expenditure by socioeconomic groups in China: an analysis of population-based panel data
Abstract
Background: Multimorbidity, the presence of two or more mental or physical chronic non-communicable diseases, is a major challenge for the health system in China, which faces unprecedented ageing of its population. Here we examined the distribution of physical multimorbidity in relation to socioeconomic status; the association between physical multimorbidity, health-care service use, and catastrophic health expenditures; and whether these associations varied by socioeconomic group and social health insurance schemes.
Methods: In this population-based, panel data analysis, we used data from three waves of the nationally representative China Health and Retirement Longitudinal Study (CHARLS) for 2011, 2013, and 2015. We included participants aged 50 years and older in 2015, who had complete follow-up for the three waves. We used 11 physical non-communicable diseases to measure physical multimorbidity and annual per-capita household consumption spending as a proxy for socioeconomic status.
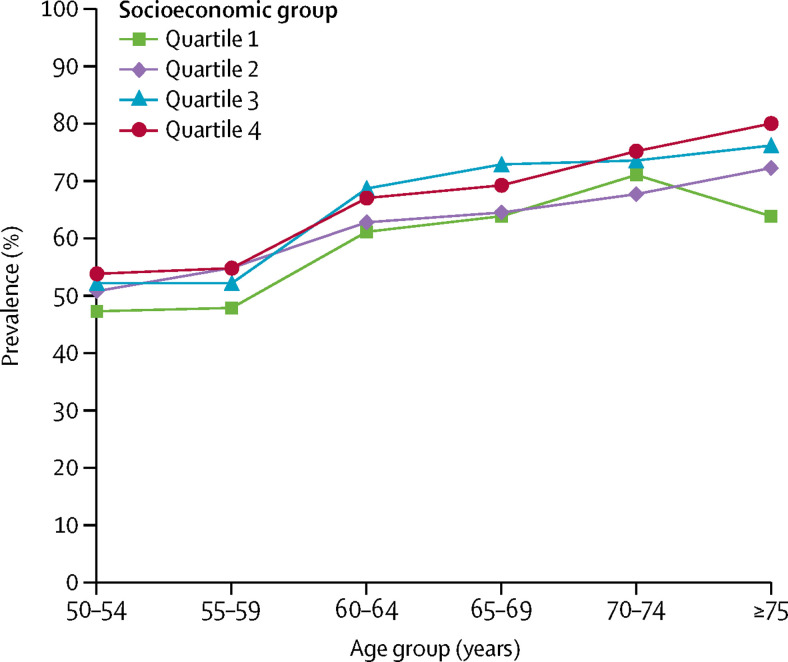
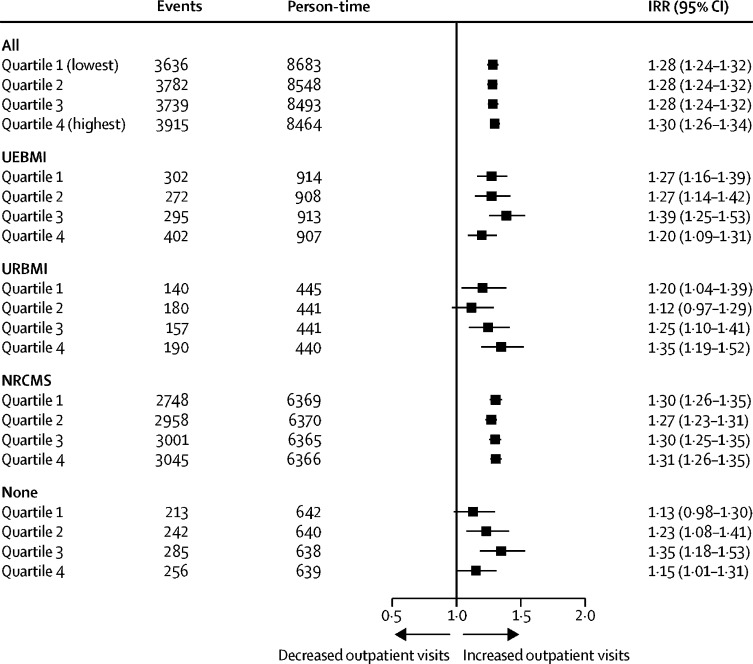
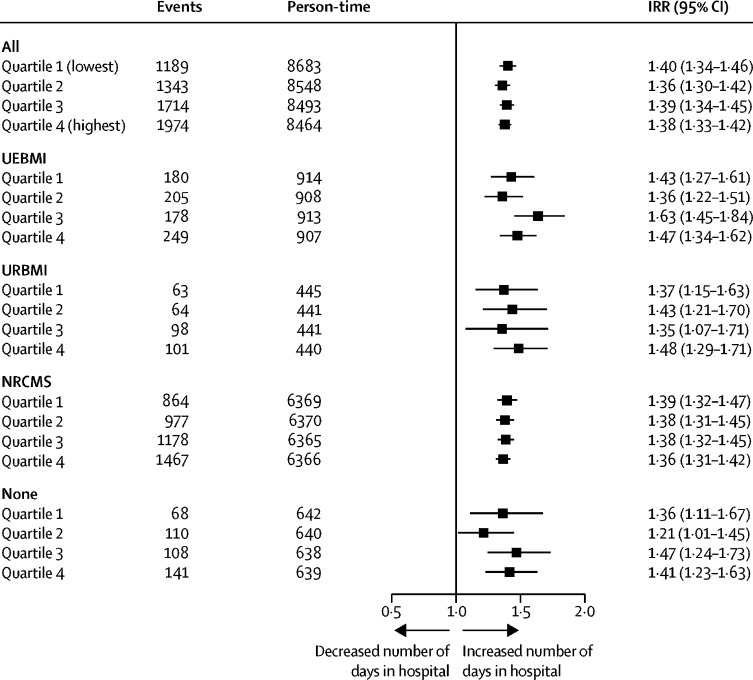
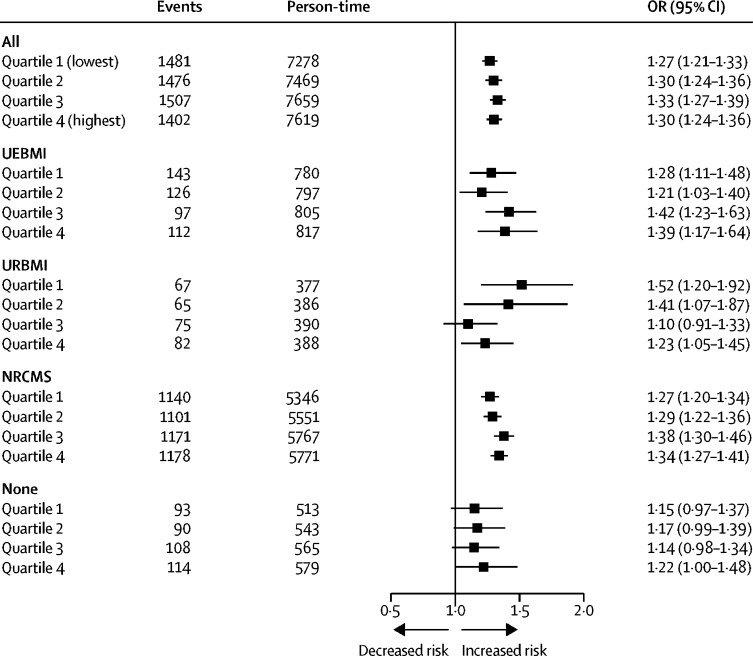
Findings: Of 17 708 participants in CHARLS, 11 817 were eligible for inclusion in our analysis. The median age of participants was 62 years (IQR 56-69) in 2015, and 5766 (48·8%) participants were male. 7320 (61·9%) eligible participants had physical multimorbidity in China in 2015. The prevalence of physical multimorbidity was increased with older age (odds ratio 2·93, 95% CI 2·71-3·15), among women (2·70, 2·04-3·57), within a higher socioeconomic group (for quartile 4 [highest group] 1·50, 1·24-1·82), and higher educational level (5·17, 3·02-8·83); however, physical multimorbidity was more common in poorer regions than in the more affluent regions. An additional chronic non-communicable disease was associated with an increase in the number of outpatient visits (incidence rate ratio 1·29, 95% CI 1·27-1·31), and number of days spent in hospital as an inpatient (1·38, 1·35-1·41). We saw similar effects in health service use of an additional chronic non-communicable disease in different socioeconomic groups and among those covered by different social health insurance programmes. Overall, physical multimorbidity was associated with a significantly increased likelihood of catastrophic health expenditure (for the overall population: odds ratio 1·29, 95% CI 1·26-1·32, adjusted for sociodemographic variables). The effect of physical multimorbidity on catastrophic health expenditures persisted even among the higher socioeconomic groups and across all health insurance programmes.
Interpretation: Concerted efforts are needed to reduce health inequalities that are due to physical multimorbidity, and its adverse economic effect in population groups in China. Social health insurance reforms must place emphasis on reducing out-of-pocket spending for patients with multimorbidity to provide greater financial risk protection.
Funding: None.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Health system reform in China: the challenges of multimorbidity.Lancet Glob Health. 2020 Jun;8(6):e750-e751. doi: 10.1016/S2214-109X(20)30225-4. Lancet Glob Health. 2020. PMID: 32446340 No abstract available.
References
-
- Yang G, Kong L, Zhao W. Emergence of chronic non-communicable diseases in China. Lancet. 2008;372:1697–1705. - PubMed
-
- Wang L, Kong L, Wu F, Bai Y, Burton R. Preventing chronic diseases in China. Lancet. 2005;366:1821–1824. - PubMed
-
- Boyd CM, Fortin M. Future of multimorbidity research: how should understanding of multimorbidity inform health system design? Public Health Rev. 2010;32:451–474.
-
- Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380:37–43. - PubMed
-
- Guthrie B, Payne K, Alderson P, McMurdo MET, Mercer SW. Adapting clinical guidelines to take account of multimorbidity. BMJ. 2012;345 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
