

Association of childhood smoking and adult mortality: prospective study of 120 000 Cuban adults
- PMID: 32446350
- PMCID: PMC7248573
- DOI: 10.1016/S2214-109X(20)30221-7
Association of childhood smoking and adult mortality: prospective study of 120 000 Cuban adults
Abstract
Background: The average age at which people start smoking has been decreasing in many countries, but insufficient evidence exists on the adult hazards of having started smoking in childhood and, especially, in early childhood. We aimed to investigate the association between smoking habits (focusing on the age when smokers started) and cause-specific premature mortality in a cohort of adults in Cuba.
Methods: For this prospective study, adults were recruited from five provinces in Cuba. Participants were interviewed (data collected included socioeconomic status, medical history, alcohol consumption, and smoking habits) and had their height, weight, and blood pressure measured. Participants were followed up until Jan 1, 2017 for cause-specific mortality; a subset was resurveyed in 2006-08. We used Cox regression to calculate adjusted rate ratios (RRs) for mortality at ages 30-69 years, comparing never-smokers with current smokers by age they started smoking and number of cigarettes smoked per day and with ex-smokers by the age at which they had quit.
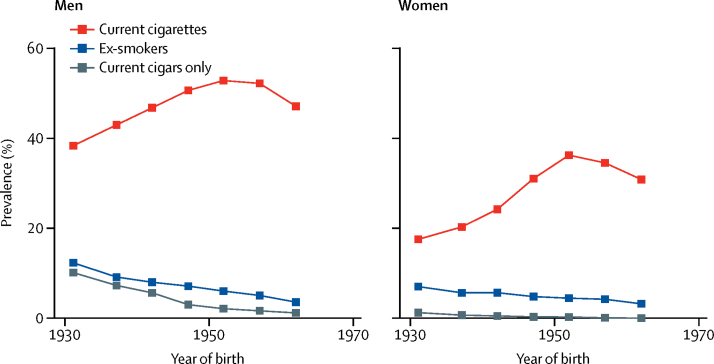
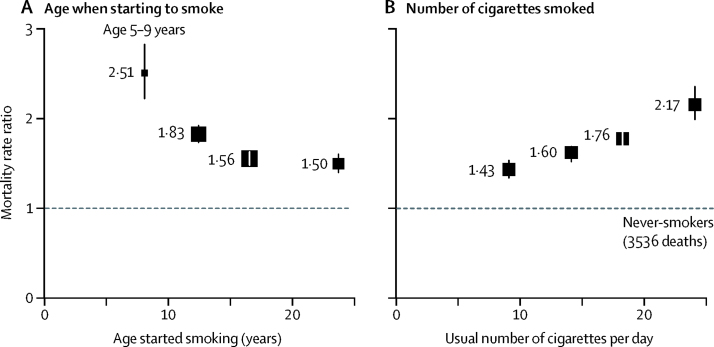
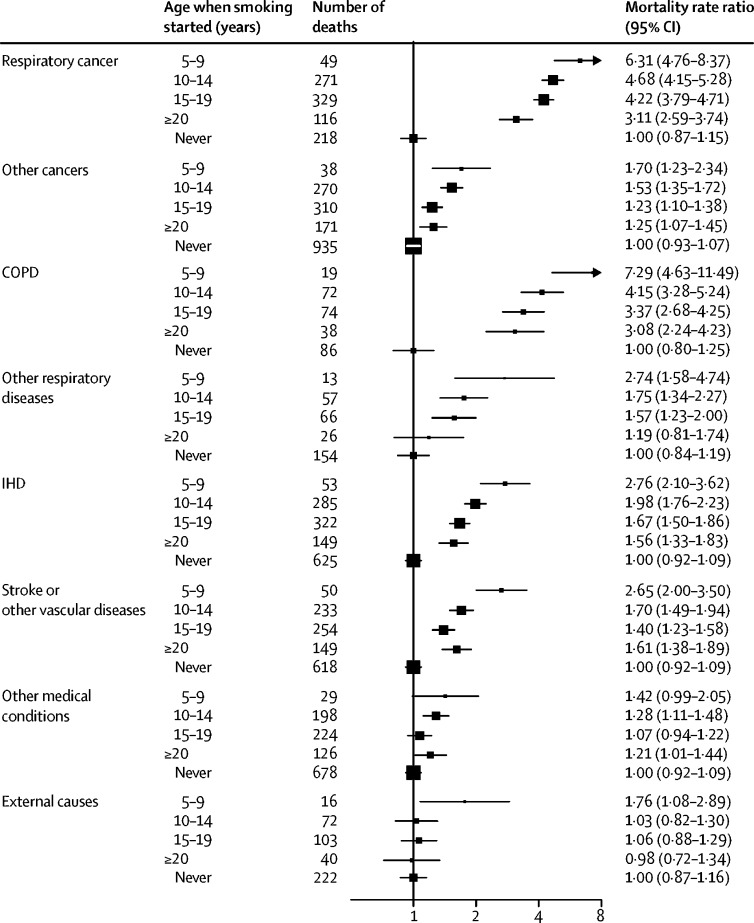
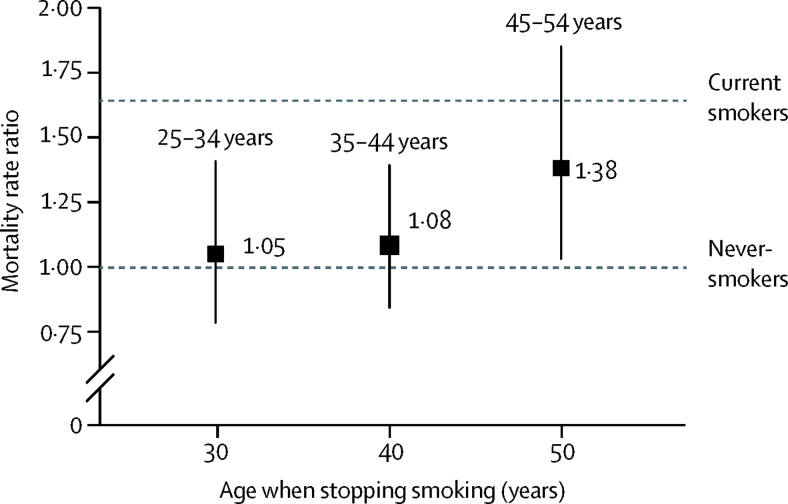
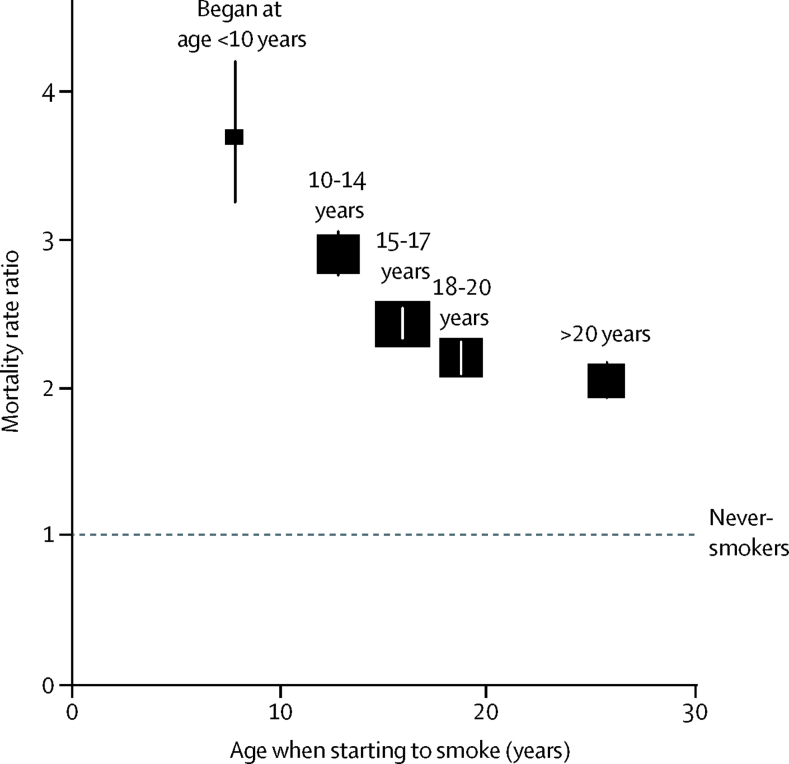
Findings: Between Jan 1, 1996, and Nov 24, 2002, 146 556 adults were recruited into the study, of whom 118 840 participants aged 30-69 years at recruitment contributed to the main analyses. 27 264 (52%) of 52 524 men and 19 313 (29%) of 66 316 women were current smokers. Most participants reported smoking cigarettes; few smoked only cigars. About a third of current cigarette smokers had started before age 15 years. Compared with never-smokers, the all-cause mortality RR was highest in participants who had started smoking at ages 5-9 years (RR 2·51, 95% CI 2·21-2·85), followed by ages 10-14 years (1·83, 1·72-1·95), 15-19 years (1·56, 1·46-1·65), and ages 20 years or older (1·50, 1·39-1·62). Smoking accounted for a quarter of all premature deaths in this population, but quitting before about age 40 years avoided almost all of the excess mortality due to smoking.
Interpretation: In this cohort of adults in Cuba, starting to smoke in childhood was common and quitting was not. Starting in childhood approximately doubled the rate of premature death (ie, before age 70 years). If this 2-fold mortality RR continues into old age, about half of participants who start smoking before age 15 years and do not stop will eventually die of complications from their habit. The greatest risks were found among adults who began smoking before age 10 years.
Funding: UK Medical Research Council, Cancer Research UK, British Heart Foundation, US Centers for Disease Control and Prevention (CDC) Foundation (with support from Amgen).
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Smoking tobacco, the major cause of death and disability in Cuba.Lancet Glob Health. 2020 Jun;8(6):e752-e753. doi: 10.1016/S2214-109X(20)30226-6. Lancet Glob Health. 2020. PMID: 32446341 No abstract available.
References
-
- WHO Global Adult Tobacco Survey. https://www.who.int/tobacco/surveillance/survey/gats/en/
-
- Bonet M, Varona P. Editorial Ciencias Medica; Havana: 2015. III Encuesta nacional de factores de riesgo y actividades preventivas de enfermedades no transmisibles. Cuba 2010–2011.
-
- US Centers for Disease Control and Prevention National Health Interview Survey. 2019. https://www.cdc.gov/nchs/nhis/index.htm
-
- Varona P, Herrera D, Garcia RG, Bonet M, Romero T, Venero SJ. Smoking-attributable mortality in cuba. MEDICC Rev. 2009;11:43–47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
