

Thinking Beyond HLH: Clinical Features of Patients with Concurrent Presentation of Hemophagocytic Lymphohistiocytosis and Thrombotic Microangiopathy
- PMID: 32447592
- PMCID: PMC7245179
- DOI: 10.1007/s10875-020-00789-4
Thinking Beyond HLH: Clinical Features of Patients with Concurrent Presentation of Hemophagocytic Lymphohistiocytosis and Thrombotic Microangiopathy
Abstract
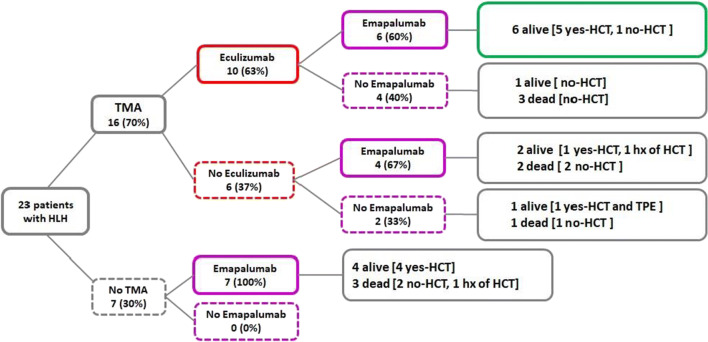
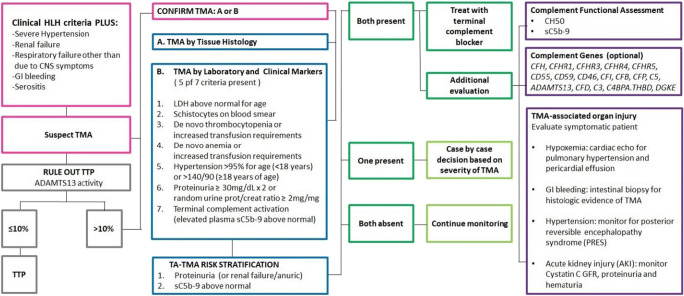
Hemophagocytic lymphohistiocytosis (HLH) is a syndrome of excessive immune system activation driven mainly by high levels of interferon gamma. The clinical presentation of HLH can have considerable overlap with other inflammatory conditions. We present a cohort of patients with therapy refractory HLH referred to our center who were found to have a simultaneous presentation of complement-mediated thrombotic microangiopathy (TMA). Twenty-three patients had therapy refractory HLH (13 primary, 4 EVB-HLH, 6 HLH without known trigger). Sixteen (69.6%) met high-risk TMA criteria. Renal failure requiring renal replacement therapy, severe hypertension, serositis, and gastrointestinal bleeding were documented only in patients with HLH who had concomitant complement-mediated TMA. Patients with HLH and without TMA required ventilator support mainly due to CNS symptoms, while those with HLH and TMA had respiratory failure predominantly associated with pulmonary hypertension, a known presentation of pulmonary TMA. Ten patients received eculizumab for complement-mediated TMA management while being treated for HLH. All patients who received the complement blocker eculizumab in addition to the interferon gamma blocker emapalumab had complete resolution of their TMA and survived. Our observations suggest co-activation of both interferon and complement pathways as a potential culprit in the evolution of thrombotic microangiopathy in patients with inflammatory disorders like refractory HLH and may offer novel therapeutic approaches for these critically ill patients. TMA should be considered in children with HLH and multi-organ failure, as an early institution of a brief course of complement blocking therapy in addition to HLH-targeted therapy may improve clinical outcomes in these patients.
Keywords: Complement; Eculizumab; Emapalumab; Hemophagocytic lymphohistiocytosis; Interferon gamma; Thrombotic microangiopathy.
Conflict of interest statement
NJG, CED, RAM, and JB have no interests to disclose. SJ and SMD have US patents pending. MBJ and AK are consultants for Sobi. ATC is on the speaker’s bureau for Sobi. None of these funding sources had any input in the study design, analysis, manuscript preparation, or decision to submit for publication.
Figures
References
-
- Buatois V, Chatel L, Cons L, Lory S, Richard F, Guilhot F, Johnson Z, Bracaglia C, De Benedetti F, de Min C, Kosco-Vilbois MH, Ferlin WG. Use of a mouse model to identify a blood biomarker for IFNgamma activity in pediatric secondary hemophagocytic lymphohistiocytosis. Transl Res. 2017;180:37–52. doi: 10.1016/j.trsl.2016.07.023. - DOI - PMC - PubMed
-
- Prencipe G, Caiello I, Pascarella A, Grom AA, Bracaglia C, Chatel L, Ferlin WG, Marasco E, Strippoli R, de Min C, De Benedetti F. Neutralization of IFN-gamma reverts clinical and laboratory features in a mouse model of macrophage activation syndrome. J Allergy Clin Immunol. 2018;141:1439–1449. doi: 10.1016/j.jaci.2017.07.021. - DOI - PubMed
-
- Bracaglia C, de Graaf K, Pires Marafon D, Guilhot F, Ferlin W, Prencipe G, Caiello I, Davi S, Schulert G, Ravelli A, Grom AA, de Min C, De Benedetti F. Elevated circulating levels of interferon-gamma and interferon-gamma-induced chemokines characterise patients with macrophage activation syndrome complicating systemic juvenile idiopathic arthritis. Ann Rheum Dis. 2017;76:166–172. doi: 10.1136/annrheumdis-2015-209020. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
