

Parameter subset reduction for patient-specific modelling of arrhythmogenic cardiomyopathy-related mutation carriers in the CircAdapt model
- PMID: 32448061
- PMCID: PMC7287326
- DOI: 10.1098/rsta.2019.0347
Parameter subset reduction for patient-specific modelling of arrhythmogenic cardiomyopathy-related mutation carriers in the CircAdapt model
Abstract
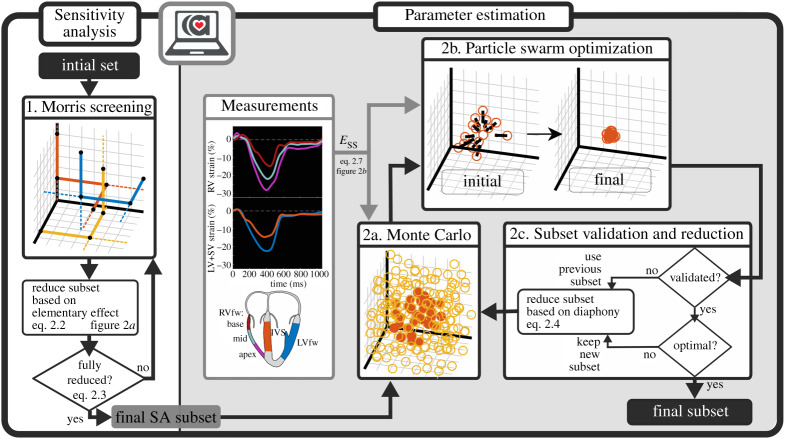
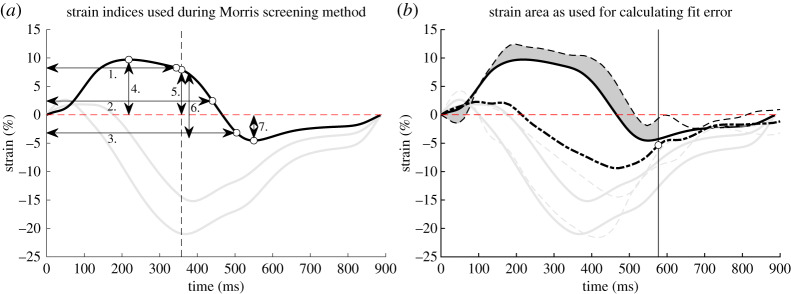
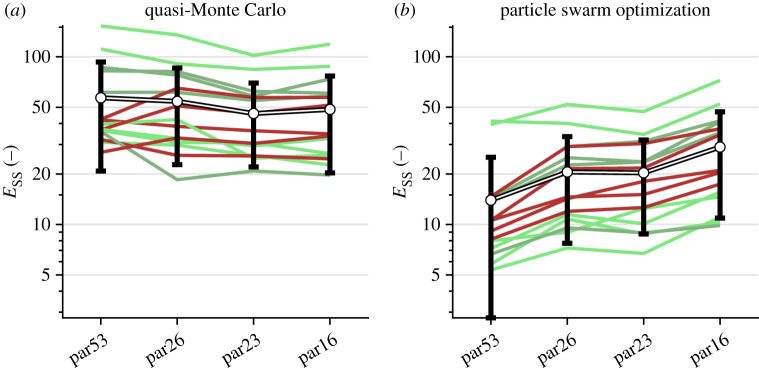
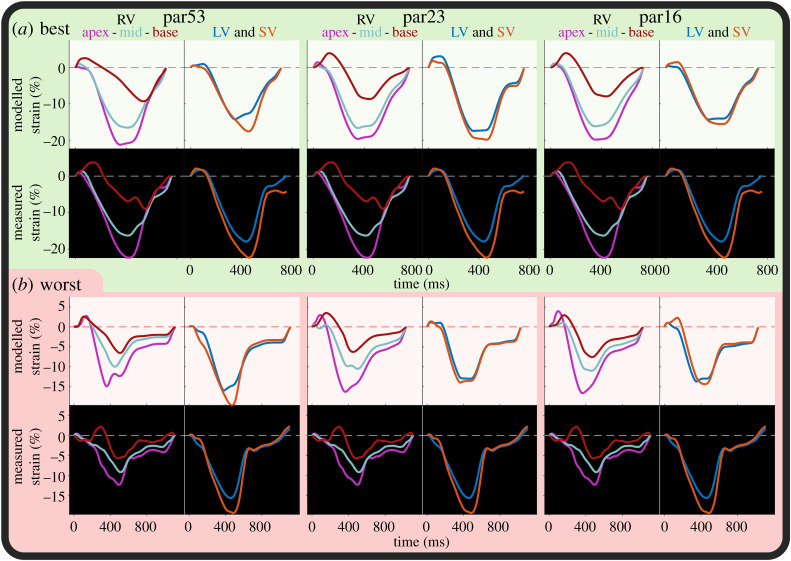
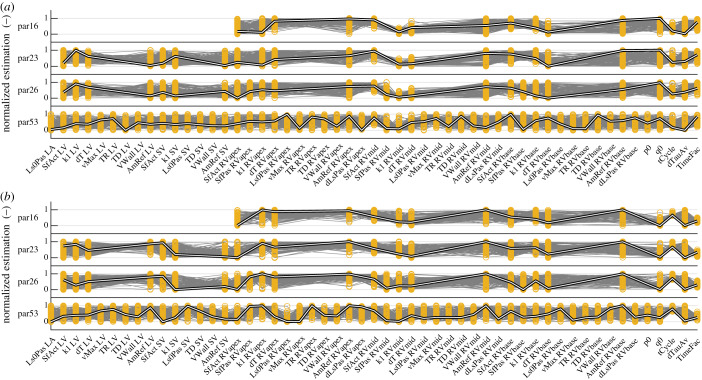
Arrhythmogenic cardiomyopathy (AC) is an inherited cardiac disease, clinically characterized by life-threatening ventricular arrhythmias and progressive cardiac dysfunction. Patient-specific computational models could help understand the disease progression and may help in clinical decision-making. We propose an inverse modelling approach using the CircAdapt model to estimate patient-specific regional abnormalities in tissue properties in AC subjects. However, the number of parameters (n = 110) and their complex interactions make personalized parameter estimation challenging. The goal of this study is to develop a framework for parameter reduction and estimation combining Morris screening, quasi-Monte Carlo (qMC) simulations and particle swarm optimization (PSO). This framework identifies the best subset of tissue properties based on clinical measurements allowing patient-specific identification of right ventricular tissue abnormalities. We applied this framework on 15 AC genotype-positive subjects with varying degrees of myocardial disease. Cohort studies have shown that atypical regional right ventricular (RV) deformation patterns reveal an early-stage AC disease. The CircAdapt model of cardiovascular mechanics and haemodynamics has already demonstrated its ability to capture typical deformation patterns of AC subjects. We, therefore, use clinically measured cardiac deformation patterns to estimate model parameters describing myocardial disease substrates underlying these AC-related RV deformation abnormalities. Morris screening reduced the subset to 48 parameters. qMC and PSO further reduced the subset to a final selection of 16 parameters, including regional tissue contractility, passive stiffness, activation delay and wall reference area. This article is part of the theme issue 'Uncertainty quantification in cardiac and cardiovascular modelling and simulation'.
Keywords: CircAdapt; Morris screening method; arrhythmogenic cardiomyopathy; parameter subset reduction; particle swarm optimization; quasi-Monte Carlo.
Conflict of interest statement
We declare we have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources