

Modified trapdoor procedures using autogenous tricortical iliac graft without preserving the broken cartilage for treatment of osteonecrosis of the femoral head: a prospective cohort study with historical controls
- PMID: 32448346
- PMCID: PMC7245755
- DOI: 10.1186/s13018-020-01691-w
Modified trapdoor procedures using autogenous tricortical iliac graft without preserving the broken cartilage for treatment of osteonecrosis of the femoral head: a prospective cohort study with historical controls
Abstract
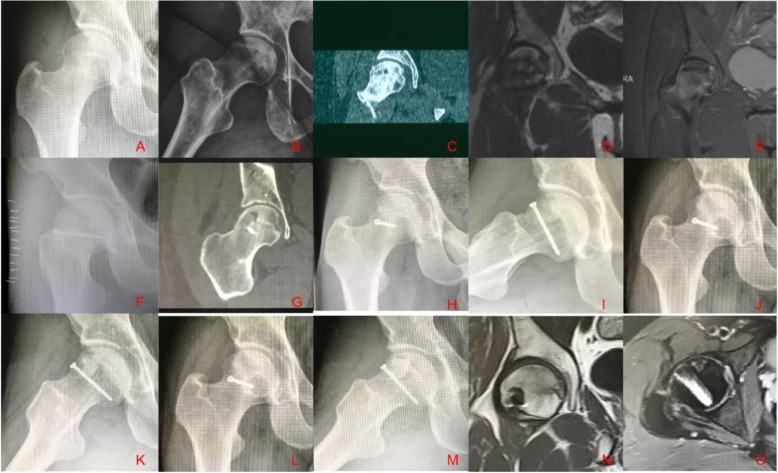
Background: The aim of the present study was to investigate clinical and radiological outcomes of autologous tricortical iliac grafting performed through a window created at the femoral head without suturing the opened articular cartilage for the treatment of osteonecrosis of the femoral head (ONFH), called modified trapdoor procedures.
Materials and methods: A total of 59 consecutive patients (67 hips; 36 males and 23 females) with ONFH were included in this study, which was conducted from April 2009 to March 2012. Patients' age ranged from 27 to 46 years old, with a mean age of 36.3 years. Harris hip scores (HHS) were used to evaluate hip function pre- and postoperatively. Anteroposterior and frog-position X-rays and magnetic resonance imaging (MRI) were conducted to assess lesion location, size, and ARCO stage. Clinical failure was defined as score < 80 points or treatment by total hip arthroplasty (THA). Radiographic failure was defined as a > 3 mm of collapse in the hip. This group was retrospectively matched according to the ARCO stage, extent, location, etiology of the lesion, average age, gender, and preoperative Harris hip score to a group of 59 patients (67 hips) who underwent the "light bulb" approach between March 2007 and April 2009.
Results: Mean follow-up was 91.2 ± 13.6 months (range, 75-115 months). Mean HHS was 91.3 ± 4.5, compared with 83.1 ± 4.5 in the "light bulb" cohort at the 6-year follow-up examination (P < 0.001). At the 6-year follow-up, for modified trapdoor procedures, five hips (8.5%) were classified as clinical failure, and three hips underwent total hip arthroplasty; seven hips were classified as (10.4%) radiographic failure. The clinical and radiographic failure of the hips treated with the modified trapdoor procedure was significantly lower compared to the hips treated with the "light bulb" procedure (P < 0.05). Survival of the joint was not significantly related to the location of the femoral head lesion between two groups; however, better clinical and radiographic results were observed in modified trapdoor procedures with size C and the ARCO stage III.
Conclusion: The present study demonstrated superior midterm clinical results in ONFH with the use of autologous tricortical iliac block graft through a femoral head window, without suturing the opened articular cartilage. The femoral head-preserving procedure was superior compared to the "light bulb" procedure treatment in patients with postcollapse osteonecrosis and large lesion.
Keywords: Bone graft; Cartilage; Hip; Osteonecrosis; Outcome; Surgical procedure.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Retrospective Long-Term Follow-Up Survival Analysis of the Management of Osteonecrosis of the Femoral Head With Pedicled Vascularized Iliac Bone Graft Transfer.J Arthroplasty. 2019 Aug;34(8):1585-1592. doi: 10.1016/j.arth.2019.03.069. Epub 2019 Apr 2. J Arthroplasty. 2019. PMID: 31031157
-
[EFFECTIVENESS OF BONE GRAFTING THROUGH WINDOWING AT FEMORAL HEAD-NECK JUNCTION FOR TREATMENT OF OSTEONECROSIS WITH SEGMENTAL COLLAPSE OF FEMORAL HEAD].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2016 Apr;30(4):397-401. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2016. PMID: 27411263 Chinese.
-
[CLINICAL APPLICATION OF THREE DIMENSIONAL PRINTED NAVIGATION TEMPLATES FOR TREATMENT OF OSTEONECROSIS OF FEMORAL HEAD WITH PEDICLED ILIAC BONE GRAFT].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2016 Mar;30(3):373-7. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2016. PMID: 27281887 Chinese.
-
Outcomes of surgical hip dislocation combined with bone graft for adolescents and younger adults with osteonecrosis of the femoral head: a case series and literature review.BMC Musculoskelet Disord. 2022 May 26;23(1):499. doi: 10.1186/s12891-022-05456-w. BMC Musculoskelet Disord. 2022. PMID: 35619082 Free PMC article. Review.
-
[Pedicled vascularized iliac bone graft for treatment of osteonecrosis of the femoral head].Oper Orthop Traumatol. 2020 Apr;32(2):127-138. doi: 10.1007/s00064-020-00650-2. Epub 2020 Feb 12. Oper Orthop Traumatol. 2020. PMID: 32052100 Review. German.
Cited by
-
Optimal parameters and Biomechanical analysis of the lightbulb technique for osteonecrosis of the femoral head: a finite element analysis.BMC Musculoskelet Disord. 2025 May 26;26(1):516. doi: 10.1186/s12891-025-08763-0. BMC Musculoskelet Disord. 2025. PMID: 40420068 Free PMC article.
-
Jack Surgery: Reconstructing Collapsed Femoral Head in Association Research Circulation Osseous Stage III Osteonecrosis: A Series of 13 Cases.Orthop Surg. 2025 Feb;17(2):644-652. doi: 10.1111/os.14298. Epub 2024 Nov 22. Orthop Surg. 2025. PMID: 39575477 Free PMC article.
-
Trapdoor Procedure for Benign Bone Lesions in the Femoral Head of Skeletally Immature Children.Orthop Surg. 2025 Jul;17(7):2183-2192. doi: 10.1111/os.70083. Epub 2025 May 29. Orthop Surg. 2025. PMID: 40442572 Free PMC article.
-
Biomechanical research of medial femoral circumflex vascularized bone-grafting in the treatment of early-to-mid osteonecrosis of the femoral head: a finite element analysis.J Orthop Surg Res. 2022 Oct 4;17(1):441. doi: 10.1186/s13018-022-03335-7. J Orthop Surg Res. 2022. PMID: 36195938 Free PMC article.
-
Phenotype-Preserving Co-culture of Osteoblasts and Chondrocytes Enhances Bone-Cartilage Interface Integration in a PRP-Augmented Scaffold.Tissue Eng Regen Med. 2025 Aug;22(6):791-803. doi: 10.1007/s13770-025-00727-8. Epub 2025 Jun 16. Tissue Eng Regen Med. 2025. PMID: 40522443 Free PMC article.
References
-
- Sonoda K, Motomura G, Kawanami S, Takayama Y, Honda H, Yamamoto T, et al. Degeneration of articular cartilage in osteonecrosis of the femoral head begins at the necrotic region after collapse: a preliminary study using T1 rho MRI. Skeletal Radiol. 2017;46:463–467. - PubMed
-
- Mont MA, Jones LC, Hungerford DS. Nontraumatic osteonecrosis of the femoral head: ten years later. J Bone Joint Surg Am. 2006;88:1117–1132. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
