

Towards a fasting-mimicking diet for critically ill patients: the pilot randomized crossover ICU-FM-1 study
- PMID: 32448392
- PMCID: PMC7245817
- DOI: 10.1186/s13054-020-02987-3
Towards a fasting-mimicking diet for critically ill patients: the pilot randomized crossover ICU-FM-1 study
Abstract
Background: In two recent randomized controlled trials, withholding parenteral nutrition early in critical illness improved outcome as compared to early up-to-calculated-target nutrition, which may be explained by beneficial effects of fasting. Outside critical care, fasting-mimicking diets were found to maintain fasting-induced benefits while avoiding prolonged starvation. It is unclear whether critically ill patients can develop a fasting response after a short-term nutrient interruption. In this randomized crossover pilot study, we investigated whether 12-h nutrient interruption initiates a metabolic fasting response in prolonged critically ill patients. As a secondary objective, we studied the feasibility of monitoring autophagy in blood samples.
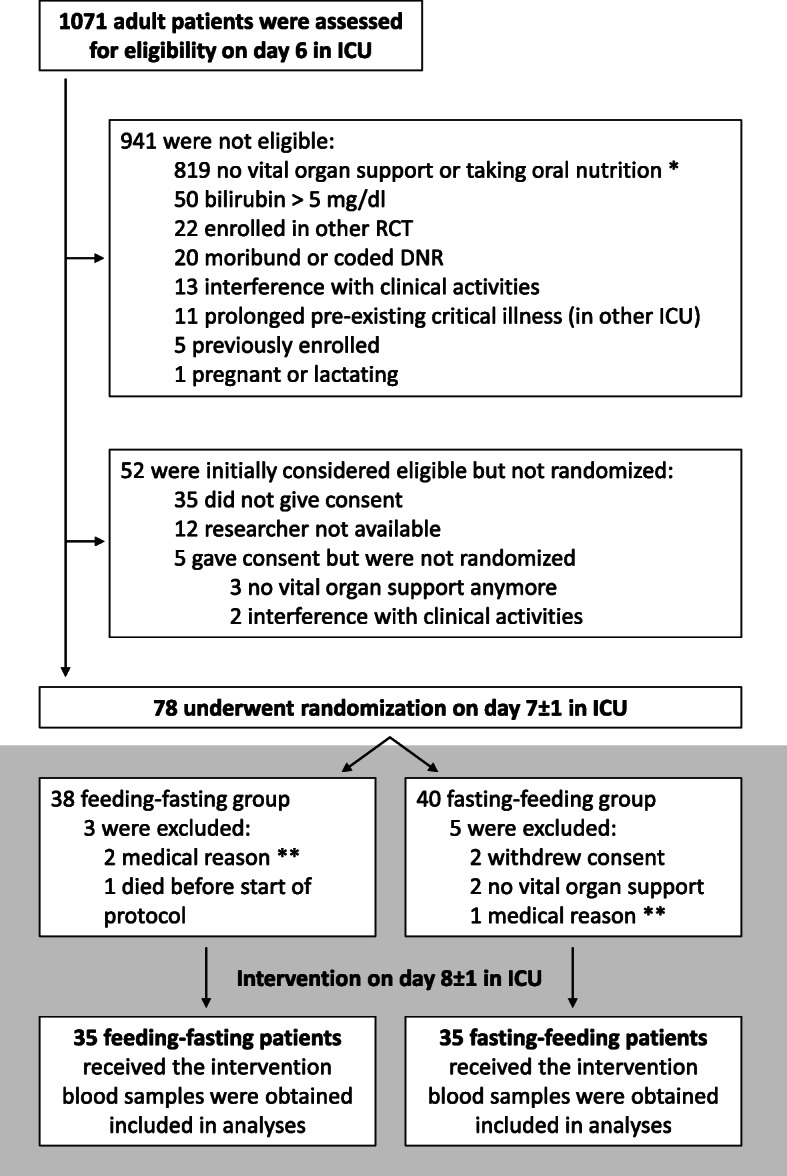
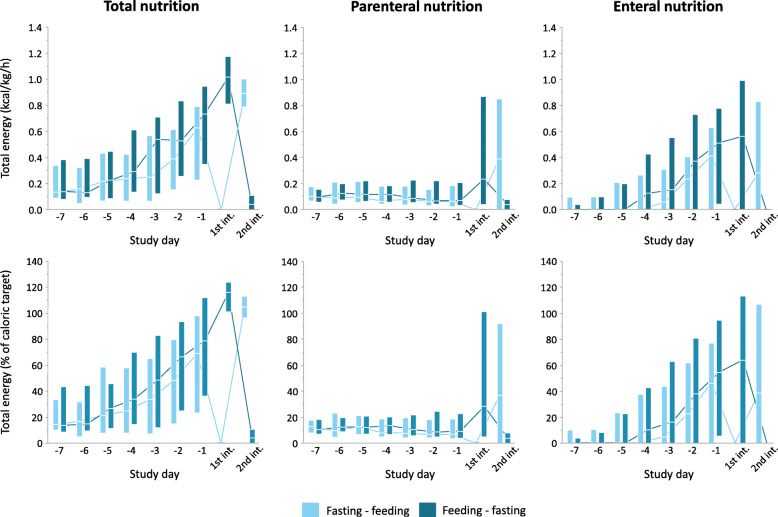
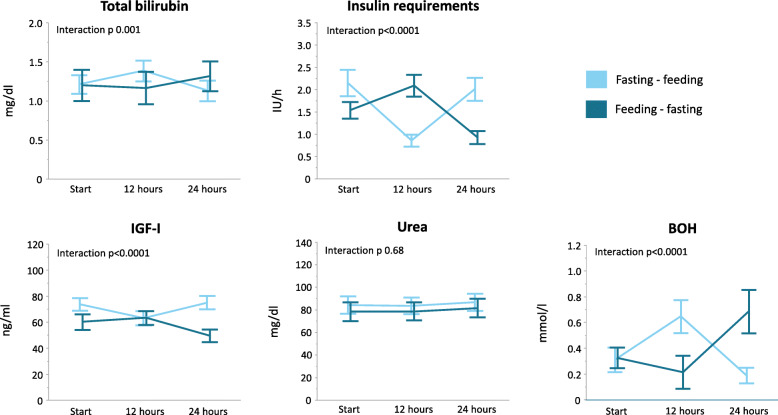
Methods: In a single-center study in 70 prolonged critically ill patients, 12-h up-to-calculated-target feeding was alternated with 12-h fasting on day 8 ± 1 in ICU, in random order. Blood samples were obtained at the start of the study, at the crossover point, and at the end of the 24-h study period. Primary endpoints were a fasting-induced increase in serum bilirubin and decrease in insulin requirements to maintain normoglycemia. Secondary outcomes included serum insulin-like growth factor I (IGF-I), serum urea, plasma beta-hydroxybutyrate (BOH), and mRNA and protein markers of autophagy in whole blood and isolated white blood cells. To obtain a healthy reference, mRNA and protein markers of autophagy were assessed in whole blood and isolated white blood cells of 23 matched healthy subjects in fed and fasted conditions. Data were analyzed using repeated-measures ANOVA, Fisher's exact test, or Mann-Whitney U test, as appropriate.
Results: A 12-h nutrient interruption significantly increased serum bilirubin and BOH and decreased insulin requirements and serum IGF-I (all p ≤ 0.001). Urea was not affected. BOH was already increased from 4 h fasting onwards. Autophagic markers in blood samples were largely unaffected by fasting in patients and healthy subjects.
Conclusions: A 12-h nutrient interruption initiated a metabolic fasting response in prolonged critically ill patients, which opens perspectives for the development of a fasting-mimicking diet. Blood samples may not be a good readout of autophagy at the tissue level.
Trial registration: ISRCTN, ISRCTN98404761. Registered 3 May 2017.
Keywords: Autophagy; Critical illness; Intensive care; Intermittent fasting; Metabolism; Nutrition.
Conflict of interest statement
None of the authors has any conflict of interest to report. Nova Biomedical and Menarini Diagnostics kindly provided the point-of-care ketone meters and accompanying analytical disposables, but were not involved in design of the study, in data collection, data analysis, writing of the manuscript, or in the decision to submit for publication.
Figures


References
-
- Alberda C, Gramlich L, Jones N, Jeejeebhoy K, Day AG, Dhaliwal R, et al. The relationship between nutritional intake and clinical outcomes in critically ill patients: results of an international multicenter observational study. Intensive Care Med. 2009;35(10):1728–1737. doi: 10.1007/s00134-009-1567-4. - DOI - PubMed
-
- Weijs PJ, Stapel SN, de Groot SD, Driessen RH, de Jong E, Girbes AR, et al. Optimal protein and energy nutrition decreases mortality in mechanically ventilated, critically ill patients: a prospective observational cohort study. JPEN J Parenter Enteral Nutr. 2012;36(1):60–68. doi: 10.1177/0148607111415109. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
