

Differentiation of retropharyngeal calcific tendinitis and retropharyngeal abscess: a case series and review of the literature
- PMID: 32449026
- PMCID: PMC7410824
- DOI: 10.1007/s00405-020-06057-w
Differentiation of retropharyngeal calcific tendinitis and retropharyngeal abscess: a case series and review of the literature
Abstract
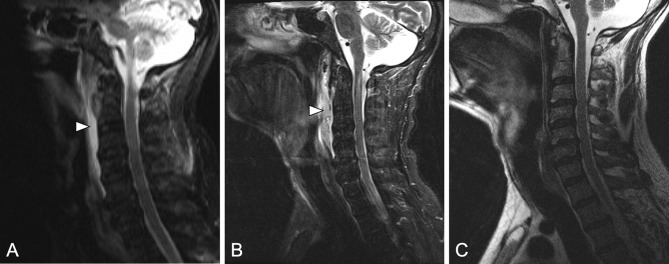
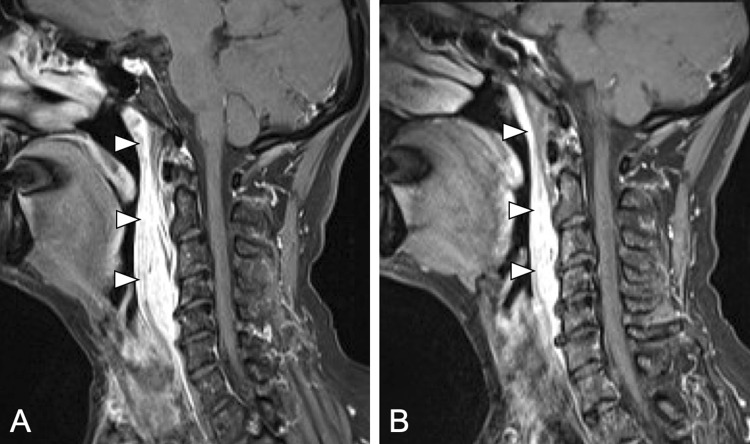
Introduction: Retropharyngeal calcific tendinitis (RCT) is a self-limiting aseptic inflammation of the tendon of the longus colli muscle, which can be clinically and radiologically misdiagnosed as abscess formation. This is a particular challenge for ENT specialists. However, articles about RCT are highly underrepresented in ENT journals and existing articles in ENT journals almost exclusively report overtreatment.
Methods: This study presents five patients, in which the diagnosis of RCT was delayed and of which one patient underwent incision and draining of a suspected retropharyngeal abscess under general anesthesia. In addition, the literature on the reported cases of RCT, between 1990 and 2020 was reviewed. For each case, epidemiological characteristics, complaints on presentation, symptoms, imaging and laboratory finding and treatment were summarized and compared to our own findings.
Results: In all the five patients, the correct diagnosis was delayed. One patient underwent incision and draining of a suspected RA under general anesthesia. All patients received antibiotic treatment. The literature review revealed a total of 116 reported cases of RCT. A total of 99 CT scans and 72 MRI showed soft tissue swelling in 89.6% and calcifications in 91.4% of the cases, 6.9% received invasive treatment.
Conclusion: This article emphasizes the importance of knowledge about RCT and its management to avoid invasive and potentially harmful treatment. The focus in establishing the correct diagnosis of RCT is the identification and correct interpretation of clinical symptoms together with the specific radiological findings.
Keywords: Neck; Neck stiffness; Pain; Prevertebral tendinitis.
Conflict of interest statement
The authors declare no conflict of interest. No funding was received for this study.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
