

Vesicoamniotic shunting for fetal megacystis in the first trimester with a Somatex® intrauterine shunt
- PMID: 32449061
- PMCID: PMC7266802
- DOI: 10.1007/s00404-020-05598-z
Vesicoamniotic shunting for fetal megacystis in the first trimester with a Somatex® intrauterine shunt
Abstract
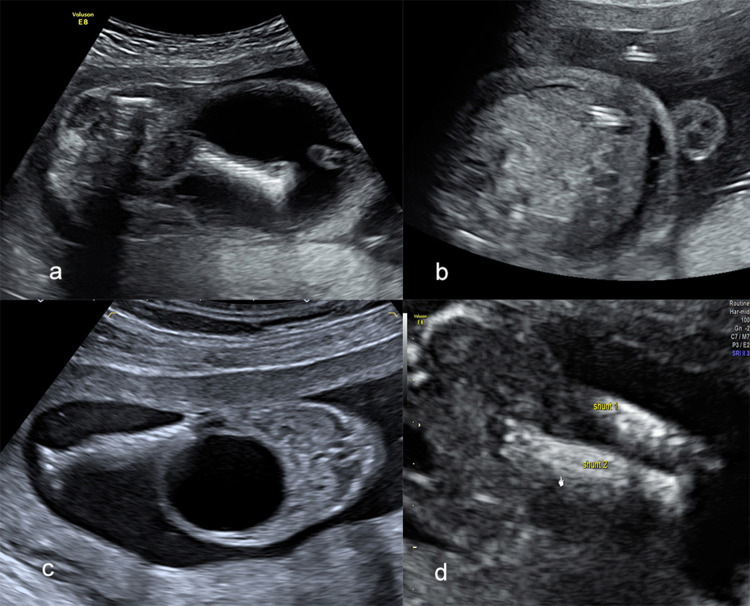
Purpose: The objective was to evaluate the feasibility of vesicoamniotic shunting (VAS) in the first trimester with the Somatex® intrauterine shunt and report on complications and neonatal outcome.
Methods: Retrospective cohort study of all VAS before 14 weeks at two tertiary fetal medicine centres from 2015 to 2018 using a Somatex® intrauterine shunt. All patients with a first trimester diagnosis of megacystis in male fetuses with a longitudinal bladder diameter of at least 15 mm were offered VAS. All patients that opted for VAS after counselling by prenatal medicine specialists, neonatologists and pediatric nephrologists were included in the study. Charts were reviewed for complications, obstetric and neonatal outcomes.
Results: Ten VAS were performed during the study period in male fetuses at a median GA of 13.3 (12.6-13.9) weeks. There were two terminations of pregnancy (TOP) due to additional malformations and one IUFD. Overall there were four shunt dislocations (40%); three of those between 25-30 weeks GA. Seven neonates were born alive at a median GA of 35.1 weeks (31.0-38.9). There was one neonatal death due to pulmonary hypoplasia. Neonatal kidney function was normal in the six neonates surviving the neonatal period. After exclusion of TOP, perinatal survival was 75%, and 85.7% if only live-born children were considered.
Conclusion: VAS in the first trimester is feasible with the Somatex® Intrauterine shunt with low fetal and maternal complication rates. Neonatal survival rates are high due to a reduction in pulmonary hypoplasia and the rate of renal failure at birth is very low. VAS can be safely offered from the late first trimester using the Somatex® intrauterine shunt.
Keywords: LUTO; Megacystis; Posterior urethral valve; Vesicoamniotic shunt.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures



References
-
- Ruano R, Sananes N, Sangi-Haghpeykar H, Hernandez-Ruano S, Moog R, Becmeur F, Zaloszyc A, Giron AM, Morin B, Favre R. Fetal intervention for severe lower urinary tract obstruction: a multicenter case-control study comparing fetal cystoscopy with vesicoamniotic shunting. Ultrasound Obstet Gynecol. 2015;45:452–458. doi: 10.1002/uog.14652. - DOI - PubMed
-
- Fievet L, Faure A, Coze S, Harper L, Panait N, Braunstein D, Carson J, Gorincour G, Chaumoitre K, Guys J-M, Alessandrini P, D’Ercole C, Merrot T. Fetal megacystis: etiologies, management, and outcome according to the trimester. Urology. 2014;84:185–190. doi: 10.1016/j.urology.2014.02.018. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
