

Imaging evaluation of COVID-19 in the emergency department
- PMID: 32449099
- PMCID: PMC7246086
- DOI: 10.1007/s10140-020-01787-0
Imaging evaluation of COVID-19 in the emergency department
Abstract
Purpose: The purpose of this study is to elucidate the chest imaging findings of suspected COVID-19 patients presenting to the emergency department and the relationship with their demographics and RT-PCR testing results.
Methods: Patients presenting to the ED between March 12 and March 28, 2020, with symptoms suspicious for COVID-19 and subsequent CXR and/or CT exam were selected. Patients imaged for other reasons with findings suspicious for COVID-19 were also included. Demographics, laboratory test results, and history were extracted from the medical record. Descriptive statistics were used to explore the relationship between imaging and these factors.
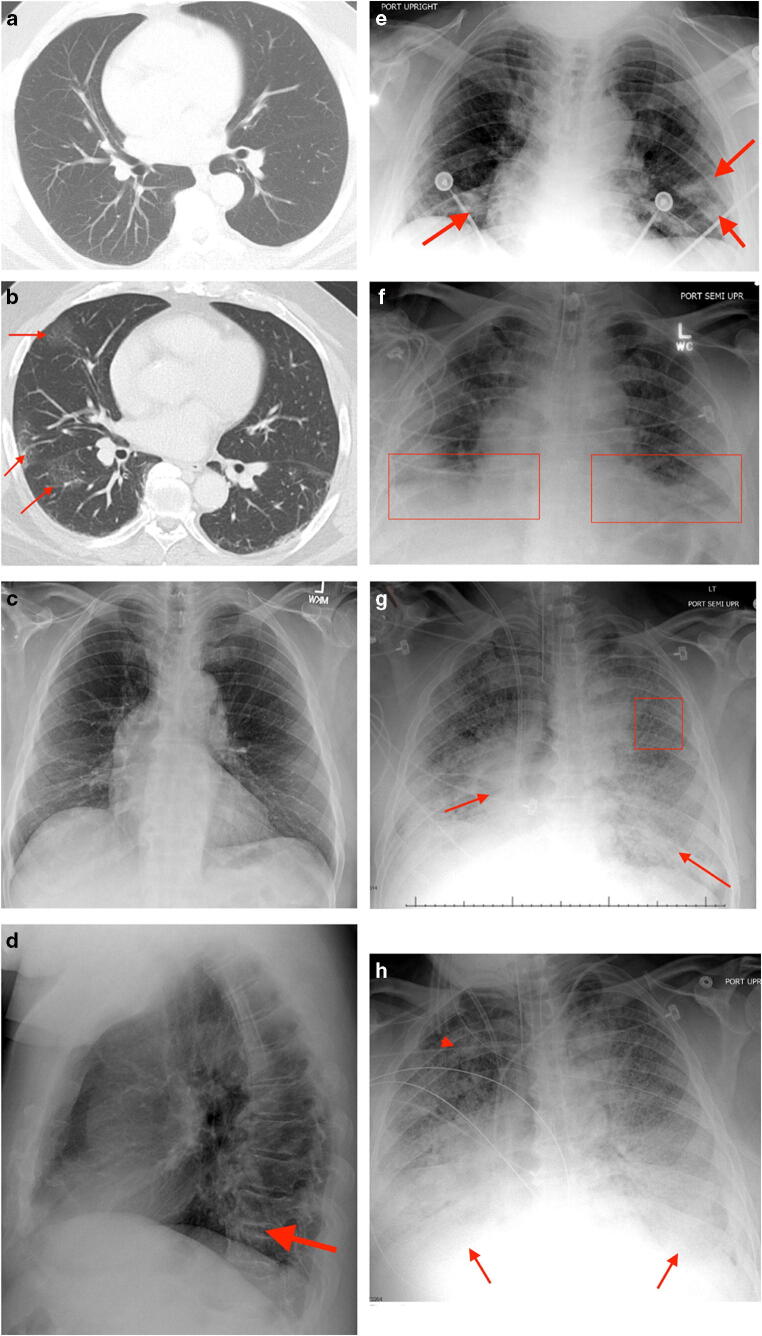
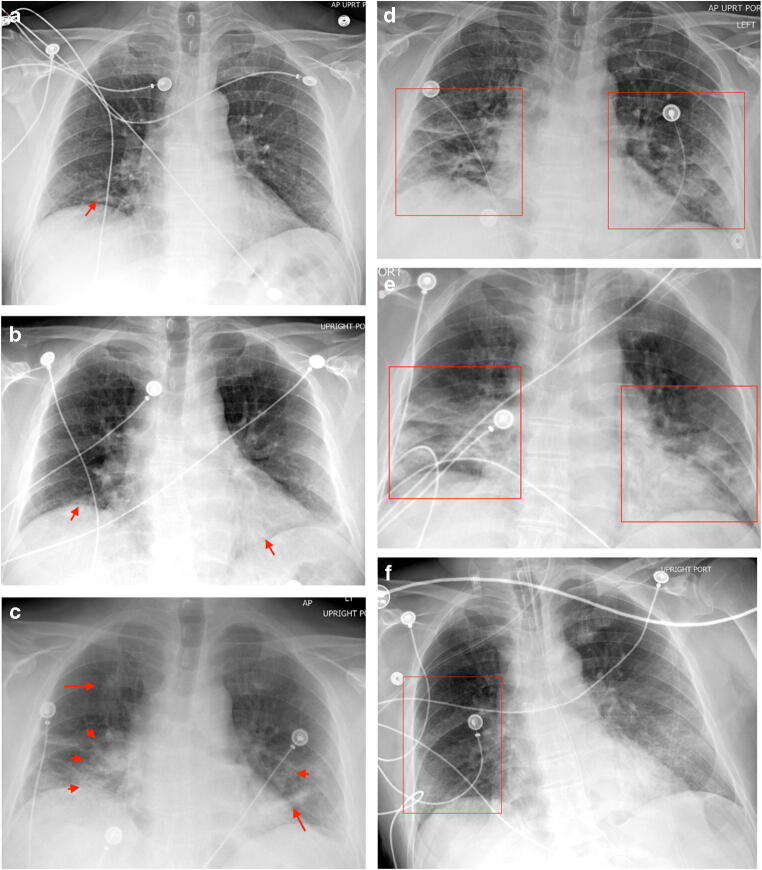
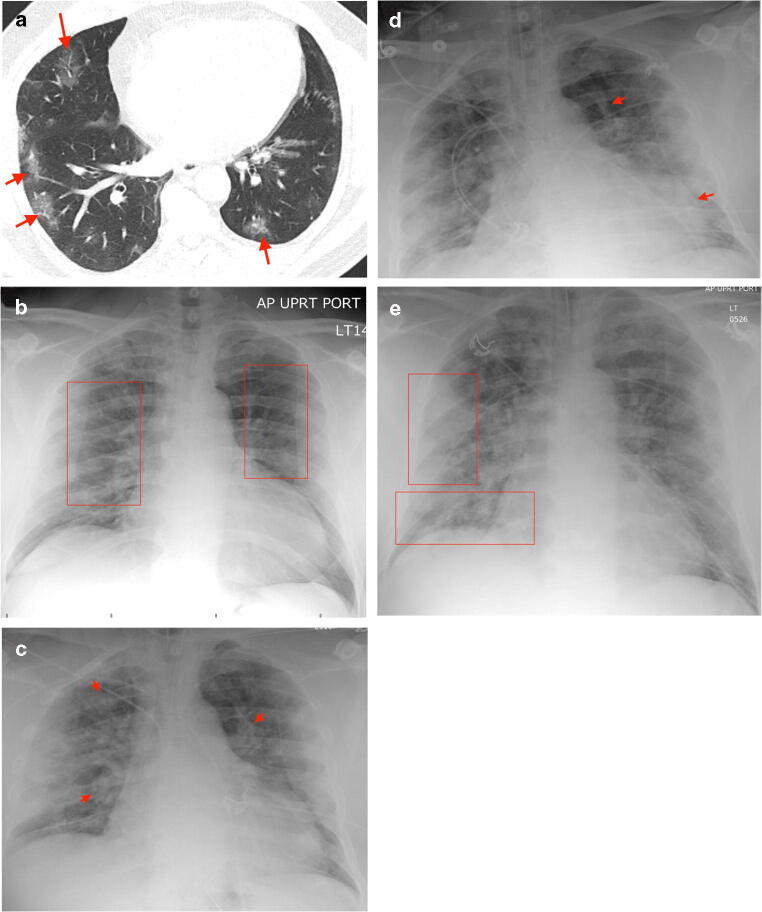
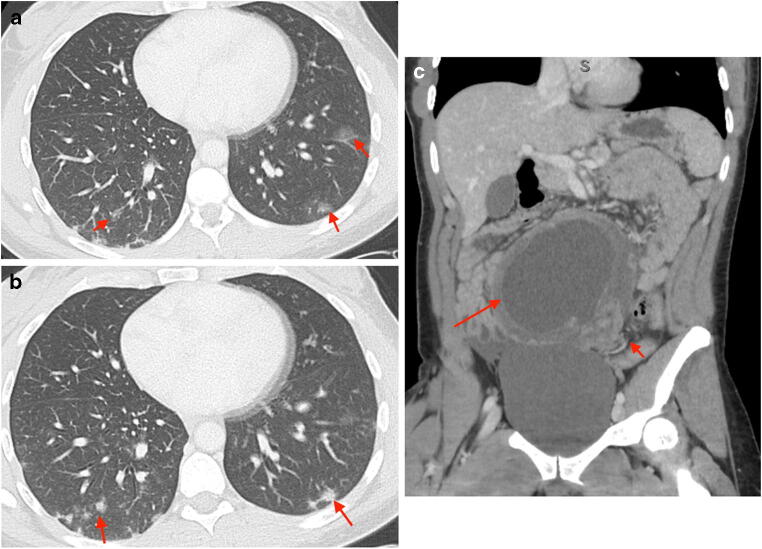
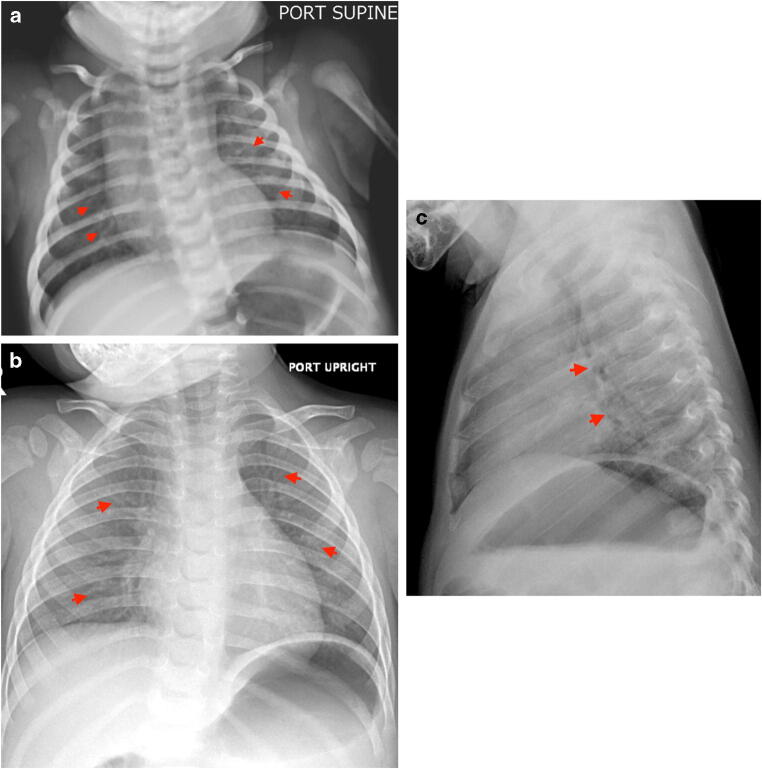
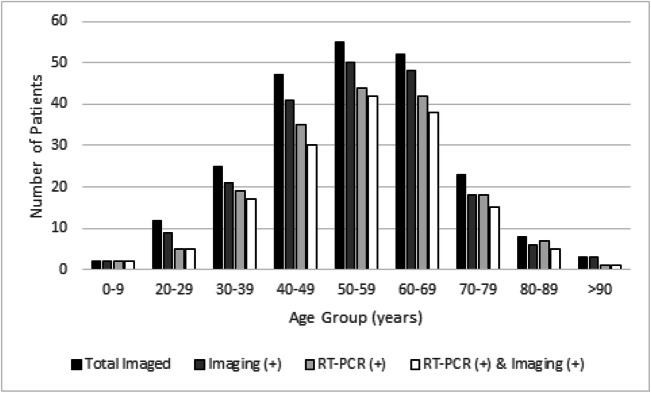
Results: A total of 227 patients from the emergency department were analyzed (224 CXRs and 25 CTs). Of the 192 patients with COVID-19 results, 173 (90.1%) had COVID-19 RT-PCR (+). Abnormal imaging (CXR, 85.7% and/or CT, 100%) was noted in 155 (89.6%) of COVID-19 RT-PCR (+) cases. The most common imaging findings were mixed airspace/interstitial opacities (39.8%) on CXR and peripheral GGOs on CT (92%). The most common demographic were African Americans (76.8%). Furthermore, 97.1% of African Americans were RT-PCR (+) compared to 65.8% of Caucasians.
Conclusion: We found a similar spectrum of thoracic imaging findings in COVID-19 patients as previous studies. The most common demographic were African Americans (76.8%). Furthermore, 97.1% of African Americans were RT-PCR (+) compared to 65.8% of Caucasians. Both CT and CXR can accurately identify COVID-19 pneumonitis in 89.6% of RT-PCR (+) cases, 89.5% of false negatives, and 72.7% of cases with no RT-PCR result.
Keywords: COVID-19; Coronavirus; Detroit; Emergency radiology; Ground glass opacities.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
