

Emergency laparotomy in the older patient: factors predictive of 12-month mortality-Salford-POPS-GS. An observational study
- PMID: 32449105
- PMCID: PMC7591437
- DOI: 10.1007/s40520-020-01578-0
Emergency laparotomy in the older patient: factors predictive of 12-month mortality-Salford-POPS-GS. An observational study
Abstract
Introduction: Although high rates of in-hospital mortality have been described in older patients undergoing emergency laparotomy (EL), less is known about longer-term outcomes in this population. We describe factors present at the time of hospital admission that influence 12-month survival in older patients.
Methods: Observational study of patients aged 75 years and over, who underwent EL at our hospital between 8th September 2014 and 30th March 2017.
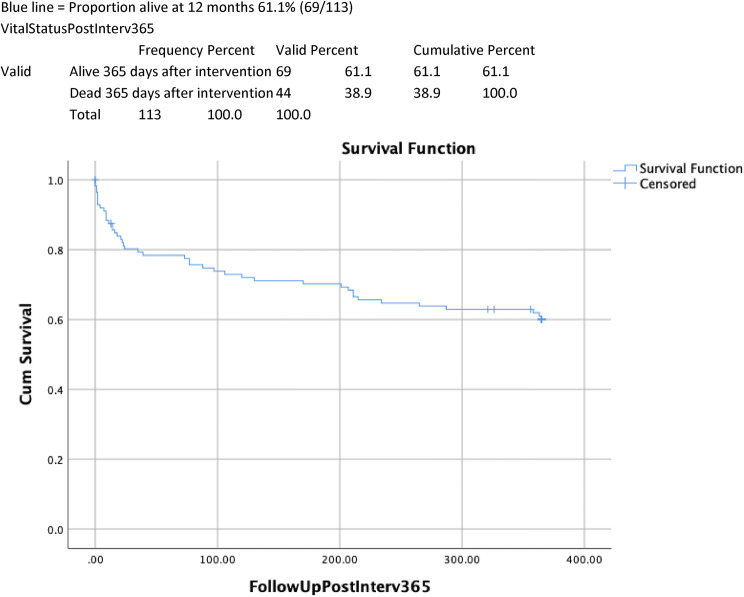
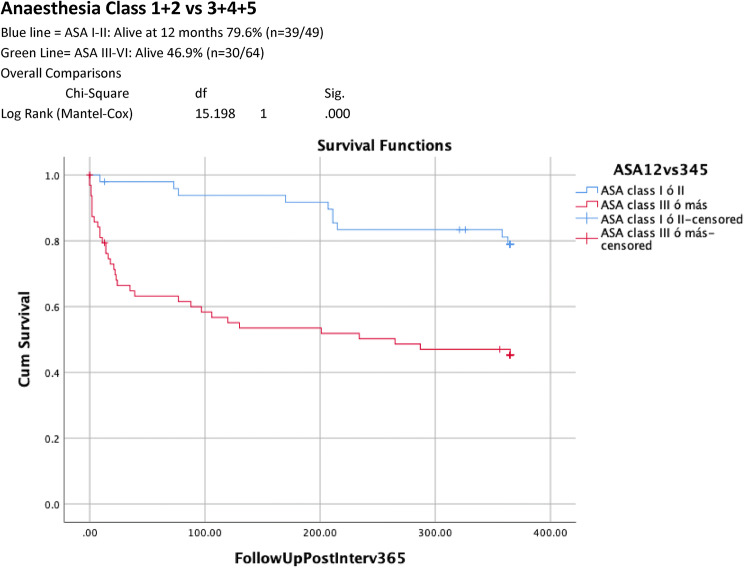
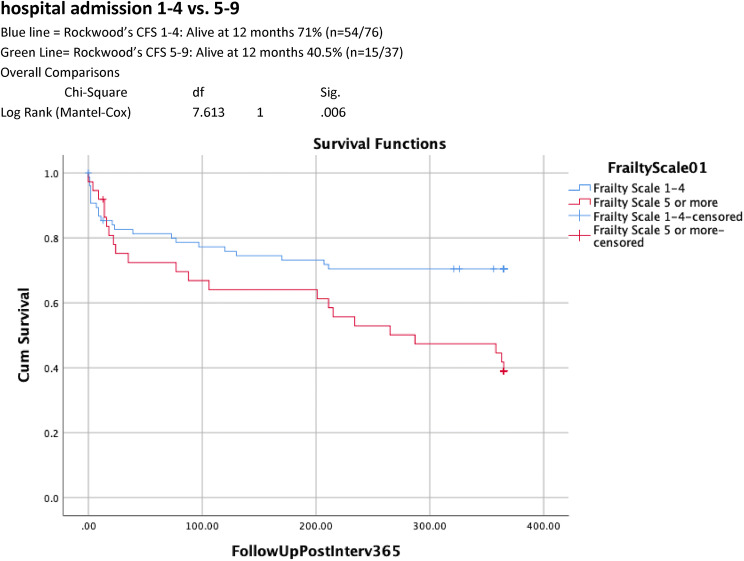
Results: 113 patients were included. Average age was 81.9 ± 4.7 years, female predominance (60/113), 3 (2.6%) lived in a care home, 103 (91.2%) and 79 (69.1%) were independent of personal and instrumental activities of daily living (ADLs) and 8 (7.1%) had cognitive impairment. Median length of stay was 16 days ± 29.9 (0-269); in-hospital mortality 22.1% (25/113), post-operative 30-day, 90-day and 12-month mortality rates 19.5% (22), 24.8% (28) and 38.9% (44). 30-day and 12-month readmission rates 5.7% (5/88) and 40.9% (36). 12-month readmission was higher in frail patients, using the Clinical Frailty Scale (CFS) score (64% 5-8 vs 31.7% 1-4, p = 0.006). Dependency for personal ADLs (6/10 (60%) dependent vs. 38/103 (36.8%) independent, p = 0.119) and cognitive impairment (5/8 (62.5%) impaired vs. 39/105 (37.1%) no impairment, p = 0.116) showed a trend towards higher 12-month mortality. On multivariate analysis, 12-month mortality was strongly associated with CFS 5-9 (HR 5.0403 (95% CI 1.719-16.982) and ASA classes III-V (HR 2.704 95% CI 1.032-7.081).
Conclusion: Frailty and high ASA class predict increased mortality at 12 months after emergency laparotomy. We advocate early engagement of multi-professional teams experienced in perioperative care of older patients.
Keywords: Comprehensive geriatric assessment; Emergency laparotomy; Frailty; Mortalitty; Older people; Surgery.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Figures
Similar articles
-
Frailty using the Clinical Frailty Scale to predict short- and long-term adverse outcomes following emergency laparotomy: meta-analysis.BJS Open. 2024 Jul 2;8(4):zrae078. doi: 10.1093/bjsopen/zrae078. BJS Open. 2024. PMID: 39166472 Free PMC article.
-
Frailty in Older Patients Undergoing Emergency Laparotomy: Results From the UK Observational Emergency Laparotomy and Frailty (ELF) Study.Ann Surg. 2021 Apr 1;273(4):709-718. doi: 10.1097/SLA.0000000000003402. Ann Surg. 2021. PMID: 31188201
-
The influence of frailty on outcomes for older adults admitted to hospital with benign biliary disease: a single-centre, observational cohort study.Ann R Coll Surg Engl. 2023 Mar;105(3):231-240. doi: 10.1308/rcsann.2021.0331. Epub 2022 May 26. Ann R Coll Surg Engl. 2023. PMID: 35616268 Free PMC article.
-
Comparison of the clinical frailty score (CFS) to the National Emergency Laparotomy Audit (NELA) risk calculator in all patients undergoing emergency laparotomy.Colorectal Dis. 2022 Jun;24(6):782-789. doi: 10.1111/codi.16089. Epub 2022 Mar 15. Colorectal Dis. 2022. PMID: 35167177 Free PMC article.
-
Frailty and cognitive impairment: Unique challenges in the older emergency surgical patient.Ann R Coll Surg Engl. 2016 Mar;98(3):165-9. doi: 10.1308/rcsann.2016.0087. Ann R Coll Surg Engl. 2016. PMID: 26890834 Free PMC article. Review.
Cited by
-
Study protocol for the COPE study: COVID-19 in Older PEople: the influence of frailty and multimorbidity on survival. A multicentre, European observational study.BMJ Open. 2020 Sep 29;10(9):e040569. doi: 10.1136/bmjopen-2020-040569. BMJ Open. 2020. PMID: 32994260 Free PMC article.
-
Association of Preoperative Risk Factors and Mortality in Older Patients following Emergency Abdominal Surgery: A Retrospective Cohort Study.Ann Geriatr Med Res. 2021 Dec;25(4):252-259. doi: 10.4235/agmr.21.0104. Epub 2021 Dec 7. Ann Geriatr Med Res. 2021. PMID: 34871476 Free PMC article.
-
Impact of preoperative frailty on outcomes in patients subjected to emergency laparotomy: a prospective study.Eur J Trauma Emerg Surg. 2025 Jan 24;51(1):34. doi: 10.1007/s00068-024-02752-z. Eur J Trauma Emerg Surg. 2025. PMID: 39853423
-
Frailty Status as a Predictor of Outcomes in Emergency Surgeries for Older Adults: A Systematic Review and Meta-Analysis.Cureus. 2025 May 15;17(5):e84160. doi: 10.7759/cureus.84160. eCollection 2025 May. Cureus. 2025. PMID: 40519493 Free PMC article. Review.
-
Frailty using the Clinical Frailty Scale to predict short- and long-term adverse outcomes following emergency laparotomy: meta-analysis.BJS Open. 2024 Jul 2;8(4):zrae078. doi: 10.1093/bjsopen/zrae078. BJS Open. 2024. PMID: 39166472 Free PMC article.
References
-
- Office for National Statistics . National Population Projections: 2016-based statistical bulletin. London: Office for National Statistics; 2017.
-
- NELA Project Team . Fifth Patient Report of the National Emergency Laparotomy Audit. London: RCoA London; 2019.
-
- Wilkinson K, Martin I, Gough M et al (2010) An age old problem. National Confidential Enquiry into Patient Outcome and Death (NCEPOD)
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
