

Intravenous fluid therapy in the perioperative and critical care setting: Executive summary of the International Fluid Academy (IFA)
- PMID: 32449147
- PMCID: PMC7245999
- DOI: 10.1186/s13613-020-00679-3
Intravenous fluid therapy in the perioperative and critical care setting: Executive summary of the International Fluid Academy (IFA)
Abstract
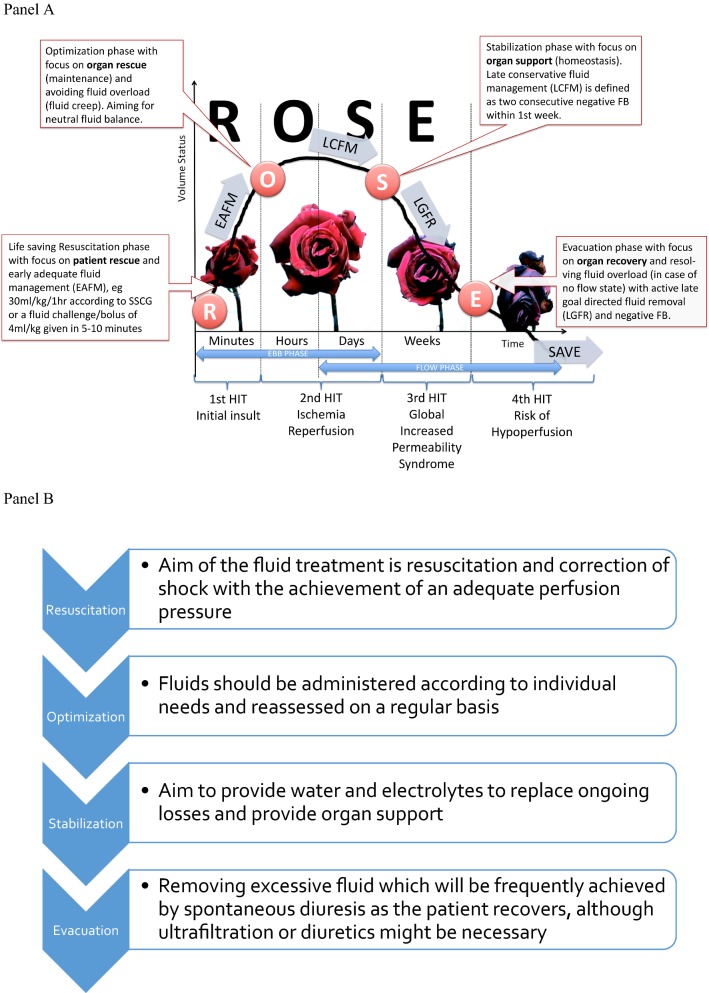
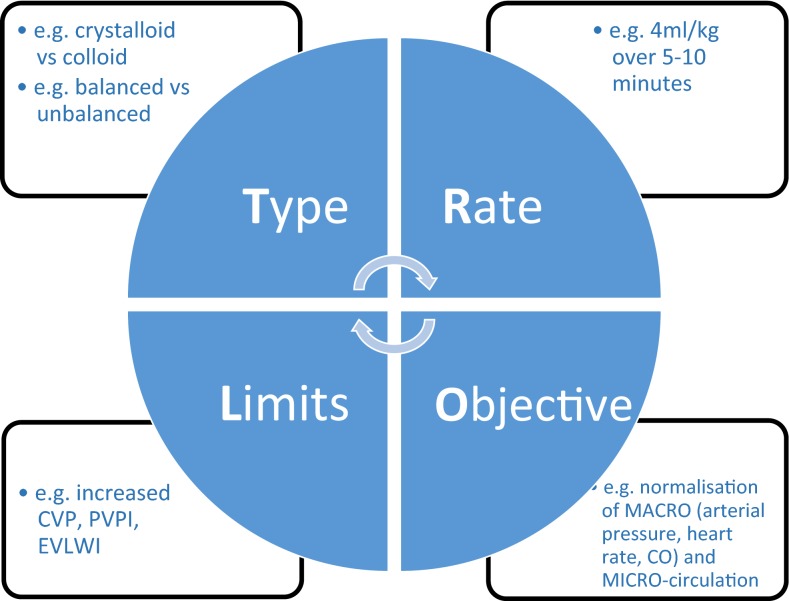
Intravenous fluid administration should be considered as any other pharmacological prescription. There are three main indications: resuscitation, replacement, and maintenance. Moreover, the impact of fluid administration as drug diluent or to preserve catheter patency, i.e., fluid creep, should also be considered. As for antibiotics, intravenous fluid administration should follow the four Ds: drug, dosing, duration, de-escalation. Among crystalloids, balanced solutions limit acid-base alterations and chloride load and should be preferred, as this likely prevents renal dysfunction. Among colloids, albumin, the only available natural colloid, may have beneficial effects. The last decade has seen growing interest in the potential harms related to fluid overloading. In the perioperative setting, appropriate fluid management that maintains adequate organ perfusion while limiting fluid administration should represent the standard of care. Protocols including a restrictive continuous fluid administration alongside bolus administration to achieve hemodynamic targets have been proposed. A similar approach should be considered also for critically ill patients, in whom increased endothelial permeability makes this strategy more relevant. Active de-escalation protocols may be necessary in a later phase. The R.O.S.E. conceptual model (Resuscitation, Optimization, Stabilization, Evacuation) summarizes accurately a dynamic approach to fluid therapy, maximizing benefits and minimizing harms. Even in specific categories of critically ill patients, i.e., with trauma or burns, fluid therapy should be carefully applied, considering the importance of their specific aims; maintaining peripheral oxygen delivery, while avoiding the consequences of fluid overload.
Keywords: Acid base; Chloride; Crystalloids; Fluid therapy; Goal-directed; Intensive care units; Maintenance; Resuscitation; Sodium; Water–electrolyte balance.
Conflict of interest statement
MLNGM is a member of the medical advisory Board of Pulsion Medical Systems (now fully integrated in Getinge, Solna, Sweden) and Serenno Medical (Tel Aviv, Israel), consults for Baxter, Maltron, ConvaTec, Acelity, Spiegelberg and Holtech Medical. NVR has received speaker’s fees from Baxter Belgium and resided in a medical advisory board organized by Baxter Healthcare, US. PE is a member of the executive committee of IFA, founder of acidbase.org, and has received speaker’s fees from Baxter Belgium and an unrestricted education grant from BBraun. TL has received speaker’s fees from Bbraun. RGH holds a research grant from Grifols for the study of 20% albumin. MM is Director of the UCL Discovery Lab. His University Chair is sponsored by Smiths Medical. He is Co-Director Duke-UCL Consortium (The Morpheus Project); a paid Consultant for Deltex Medical and Edwards Lifesciences; a Director of the Bloomsbury Innovation Group (BiG); a Director and Chair of Evidence Based Perioperative Medicine (EBPOM) Community Interest Company; Share holder and Scientific Advisor Medical Defense Technologies LLC (Gastrostim and Entarik); Share holder and Director Clinical Hydration Solutions ltd (Patent holder “QUENCH”); GIFTASUP guidelines—Senior Author; NICE—Expert Advsior IV Fluids—Guideline 174. PC has received speaker’s fees from Bbraun, Baxter, and Octapharma and resided in the Critical Care Scientific Advisory Committee organized by Werfen group, and in a medical advisory board organized by Baxter. The other authors have no potential conflict of interest with regard to the content of this review paper.
Figures
References
-
- Van Regenmortel N, Jorens PG, Malbrain ML. Fluid management before, during and after elective surgery. Curr Opin Crit Care. 2014;20(4):390–395. - PubMed
-
- Perner A, Haase N, Guttormsen AB, Tenhunen J, Klemenzson G, Aneman A, et al. Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis. N Engl J Med. 2012;367(2):124–134. - PubMed
-
- Langer T, Santini A, Scotti E, Van Regenmortel N, Malbrain ML, Caironi P. Intravenous balanced solutions: from physiology to clinical evidence. Anaesthesiol Intensive Ther. 2015;47(Spec No):s78–s88. - PubMed
-
- Malbrain ML, Van Regenmortel N, Owczuk R. It is time to consider the four D’s of fluid management. Anaesthesiol Intensive Ther. 2015;47(Spec No):s1–s5. - PubMed
-
- Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney injury in critically ill adults. JAMA. 2012;308(15):1566–1572. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Research Materials
