

The Unrecognized Prevalence of Primary Aldosteronism: A Cross-sectional Study
- PMID: 32449886
- PMCID: PMC7459427
- DOI: 10.7326/M20-0065
The Unrecognized Prevalence of Primary Aldosteronism: A Cross-sectional Study
Abstract
Background: Primary aldosteronism is a nonsuppressible renin-independent aldosterone production that causes hypertension and cardiovascular disease.
Objective: To characterize the prevalence of nonsuppressible renin-independent aldosterone production, as well as biochemically overt primary aldosteronism, in relation to blood pressure.
Design: Cross-sectional study.
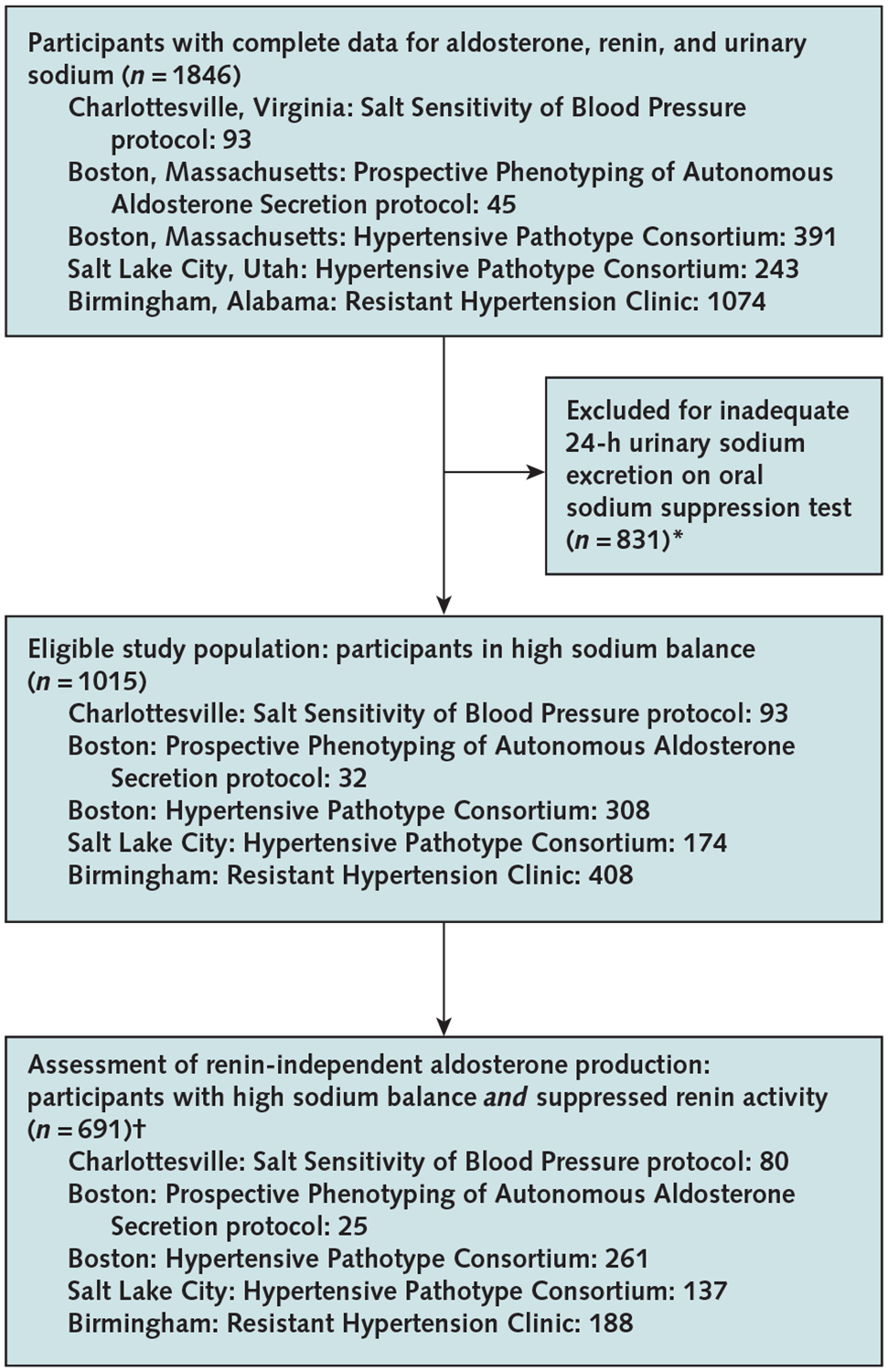
Setting: 4 U.S. academic medical centers.
Participants: Participants with normotension (n = 289), stage 1 hypertension (n = 115), stage 2 hypertension (n = 203), and resistant hypertension (n = 408).
Measurements: Participants completed an oral sodium suppression test, regardless of aldosterone or renin levels, as a confirmatory diagnostic for primary aldosteronism and to quantify the magnitude of renin-independent aldosterone production. Urinary aldosterone was measured in participants in high sodium balance with suppressed renin activity. Biochemically overt primary aldosteronism was diagnosed when urinary aldosterone levels were higher than 12 μg/24 h.
Results: Every blood pressure category had a continuum of renin-independent aldosterone production, where greater severity of production was associated with higher blood pressure, kaliuresis, and lower serum potassium levels. Mean adjusted levels of urinary aldosterone were 6.5 μg/24 h (95% CI, 5.2 to 7.7 μg/24 h) in normotension, 7.3 μg/24 h (CI, 5.6 to 8.9 μg/24 h) in stage 1 hypertension, 9.5 μg/24 h (CI, 8.2 to 10.8 μg/24 h) in stage 2 hypertension, and 14.6 μg/24 h (CI, 12.9 to 16.2 μg/24 h) in resistant hypertension; corresponding adjusted prevalence estimates for biochemically overt primary aldosteronism were 11.3% (CI, 5.9% to 16.8%), 15.7% (CI, 8.6% to 22.9%), 21.6% (CI, 16.1% to 27.0%), and 22.0% (CI, 17.2% to 26.8%). The aldosterone-renin ratio had poor sensitivity and negative predictive value for detecting biochemically overt primary aldosteronism.
Limitation: Prevalence estimates rely on arbitrary and conventional thresholds, and the study population may not represent nationwide demographics.
Conclusion: The prevalence of primary aldosteronism is high and largely unrecognized. Beyond this categorical definition of primary aldosteronism, there is a prevalent continuum of renin-independent aldosterone production that parallels the severity of hypertension. These findings redefine the primary aldosteronism syndrome and implicate it in the pathogenesis of "essential" hypertension.
Primary funding source: National Institutes of Health.
Keywords: Aldosterone; Blood pressure; Cardiovascular diseases; Excretion; Hypertension; Potassium; Resistant hypertension; Salts; Sensitivity; Sodium.
Conflict of interest statement
Figures

Comment in
-
Primary Aldosteronism: At the Tipping Point.Ann Intern Med. 2020 Jul 7;173(1):65-66. doi: 10.7326/M20-1758. Epub 2020 May 26. Ann Intern Med. 2020. PMID: 32449882 No abstract available.
-
The Unrecognized Prevalence of Primary Aldosteronism.Ann Intern Med. 2020 Oct 20;173(8):683. doi: 10.7326/L20-1097. Ann Intern Med. 2020. PMID: 33075250 Free PMC article. No abstract available.
-
The Unrecognized Prevalence of Primary Aldosteronism.Ann Intern Med. 2020 Oct 20;173(8):681. doi: 10.7326/L20-1096. Ann Intern Med. 2020. PMID: 33075252 No abstract available.
-
The Unrecognized Prevalence of Primary Aldosteronism.Ann Intern Med. 2020 Oct 20;173(8):682-683. doi: 10.7326/L20-1095. Ann Intern Med. 2020. PMID: 33075253 No abstract available.
-
The Unrecognized Prevalence of Primary Aldosteronism.Ann Intern Med. 2020 Oct 20;173(8):681-682. doi: 10.7326/L20-1094. Ann Intern Med. 2020. PMID: 33075254 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL086907/HL/NHLBI NIH HHS/United States
- R01 HL128189/HL/NHLBI NIH HHS/United States
- R01 HL113004/HL/NHLBI NIH HHS/United States
- R01 DK107407/DK/NIDDK NIH HHS/United States
- R01 HL144779/HL/NHLBI NIH HHS/United States
- P30 DK079626/DK/NIDDK NIH HHS/United States
- T32 HL007457/HL/NHLBI NIH HHS/United States
- R01 HL136567/HL/NHLBI NIH HHS/United States
- R01 HL085224/HL/NHLBI NIH HHS/United States
- R01 HL114765/HL/NHLBI NIH HHS/United States
- P01 HL074940/HL/NHLBI NIH HHS/United States
- P50 HL055000/HL/NHLBI NIH HHS/United States
- R01 DK115392/DK/NIDDK NIH HHS/United States
- R01 DK106618/DK/NIDDK NIH HHS/United States
- T32 HL007604/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical