

Coronaviruses pathogenesis, comorbidities and multi-organ damage - A review
- PMID: 32450165
- PMCID: PMC7243768
- DOI: 10.1016/j.lfs.2020.117839
Coronaviruses pathogenesis, comorbidities and multi-organ damage - A review
Abstract
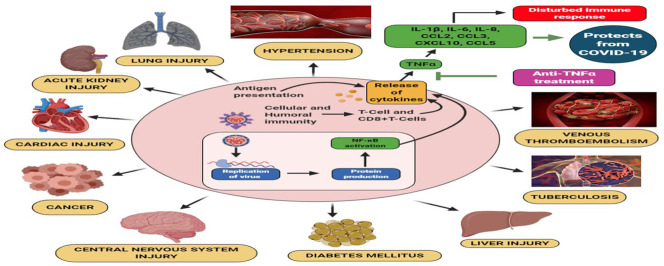
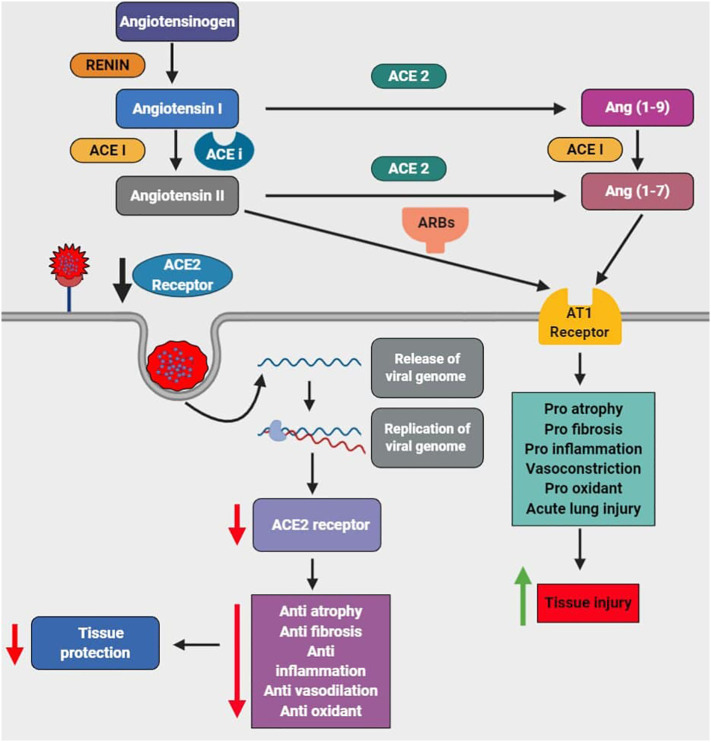
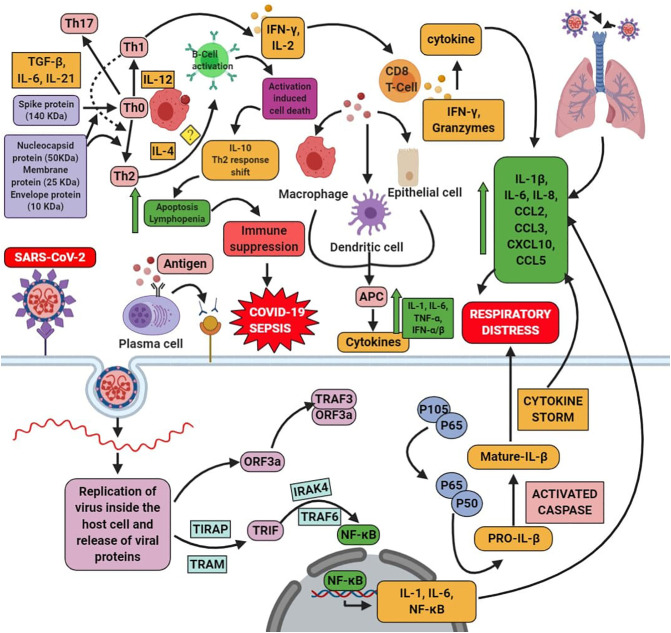
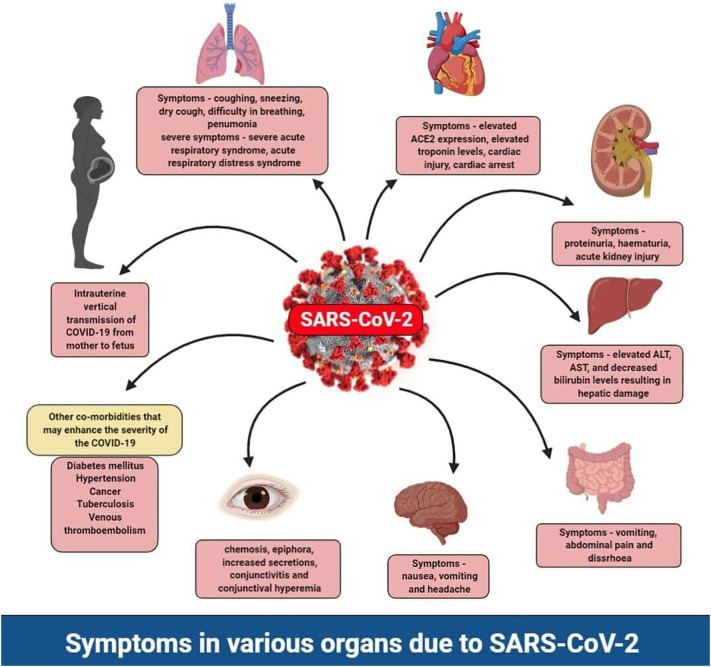
Human coronaviruses, especially COVID-19, is an emerging pandemic infectious disease with high morbidity and mortality. Coronaviruses are associated with comorbidities, along with the symptoms of it. SARS-CoV-2 is one of the highly pathogenic coronaviruses that causes a high death rate compared to the SARS-CoV and MERS. In this review, we focused on the mechanism of coronavirus with comorbidities and impairment in multi-organ function. The main dysfunction upon coronavirus infection is damage to alveolar and acute respiratory failure. It is associated with the other organ damage such as cardiovascular risk via an increased level of hypertension through ACE2, gastrointestinal dysfunction, chronic kidney disease, diabetes mellitus, liver dysfunction, lung injury, CNS risk, ocular risks such as chemosis, conjunctivitis, and conjunctival hyperemia, cancer risk, venous thromboembolism, tuberculosis, aging, and cardiovascular dysfunction and reproductive risk. Along with this, we have discussed the immunopathology and coronaviruses at a molecular level and therapeutic approaches for the coronavirus infection. The comorbidities and multi-organ failure of COVID-19 have been explained at a molecular level along with the base of the SARS-CoV and MERS-CoV. This review would help us to understand the comorbidities associated with the coronaviruses with multi-organ damage.
Keywords: COVID-19; Comorbidities; Multi-organ failure and immunopathology; SARS-CoV-2.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Cascella M., Rajnik M., Cuomo A., Dulebohn S.C., Di Napoli R. StatPearls Publishing; 2020. Features, Evaluation and Treatment Coronavirus (COVID-19), StatPearls. Internet. - PubMed
-
- Ngandu T., Lehtisalo J., Solomon A., Levälahti E., Ahtiluoto S., Antikainen R., Bäckman L., Hänninen T., Jula A., Laatikainen T. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. Lancet. 2015;385:2255–2263. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
