

Calculation of Stop Ages for Colorectal Cancer Screening Based on Comorbidities and Screening History
- PMID: 32450362
- PMCID: PMC7982961
- DOI: 10.1016/j.cgh.2020.05.038
Calculation of Stop Ages for Colorectal Cancer Screening Based on Comorbidities and Screening History
Abstract
Background & aims: Routine screening for colorectal cancer typically is recommended until age 74 years. Although it has been proposed that a screening stop age could be determined based on sex and comorbidity, less is known about the impact of screening history. We investigated the effects of screening history on the selection of an optimal age to stop screening.
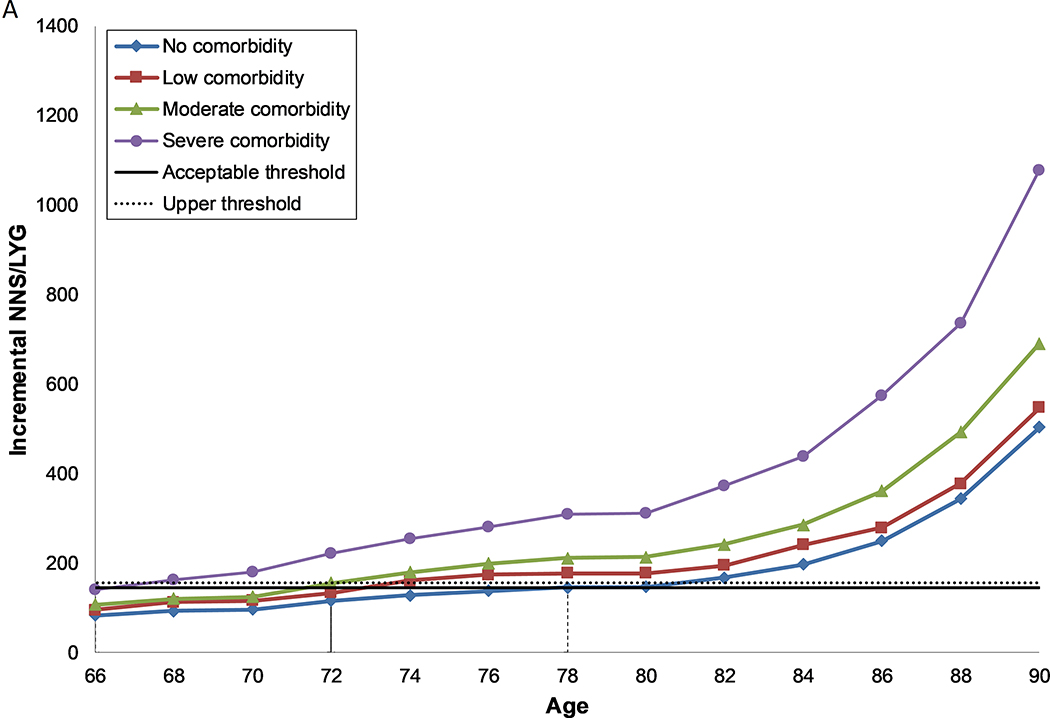
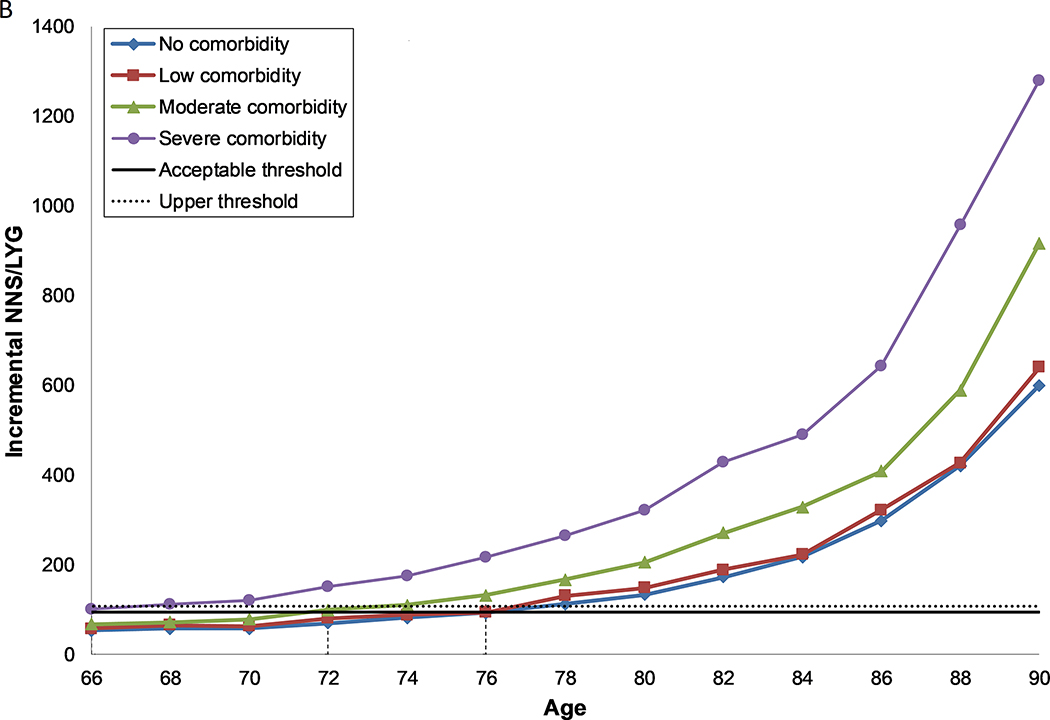
Methods: We used the Microsimulation Screening Analysis-Colon model to estimate the harms and benefits of screening with biennial fecal immunochemical tests by sex, comorbidity status, and screening history. The optimal screening stop age was determined based on the incremental number needed for 1 additional life-year per 1000 screened individuals compared with the threshold provided by stopping screening at 76 years in the average-health population with a perfect screening history (attended all required screening, diagnostic, and follow-up tests) to biennial fecal immunochemical testing from age 50 years.
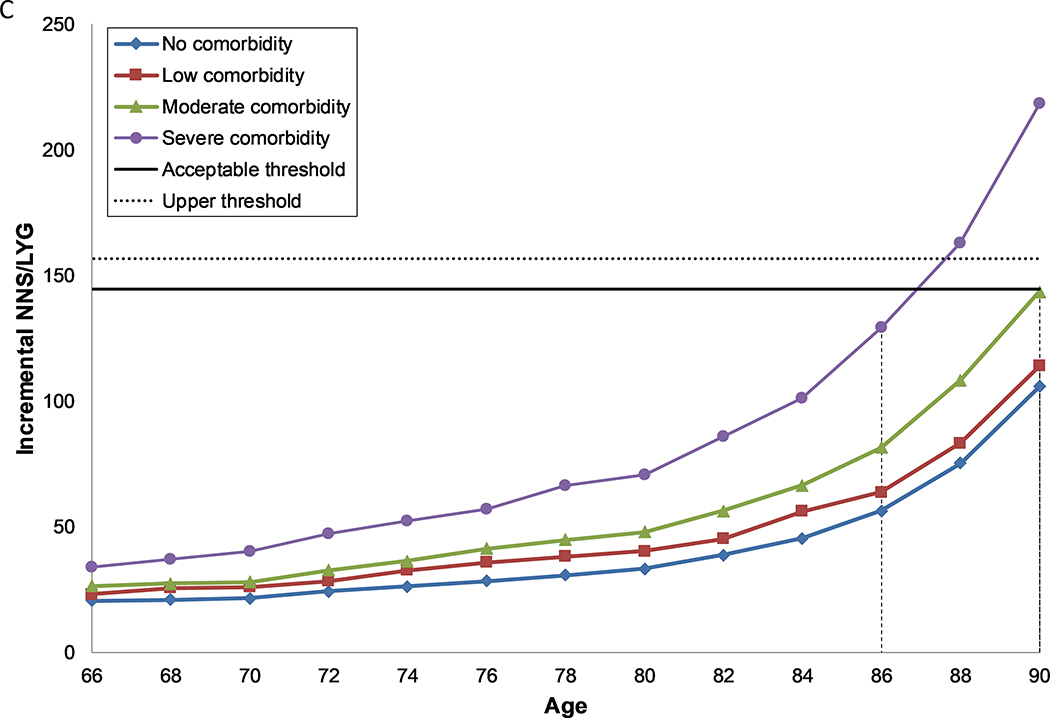
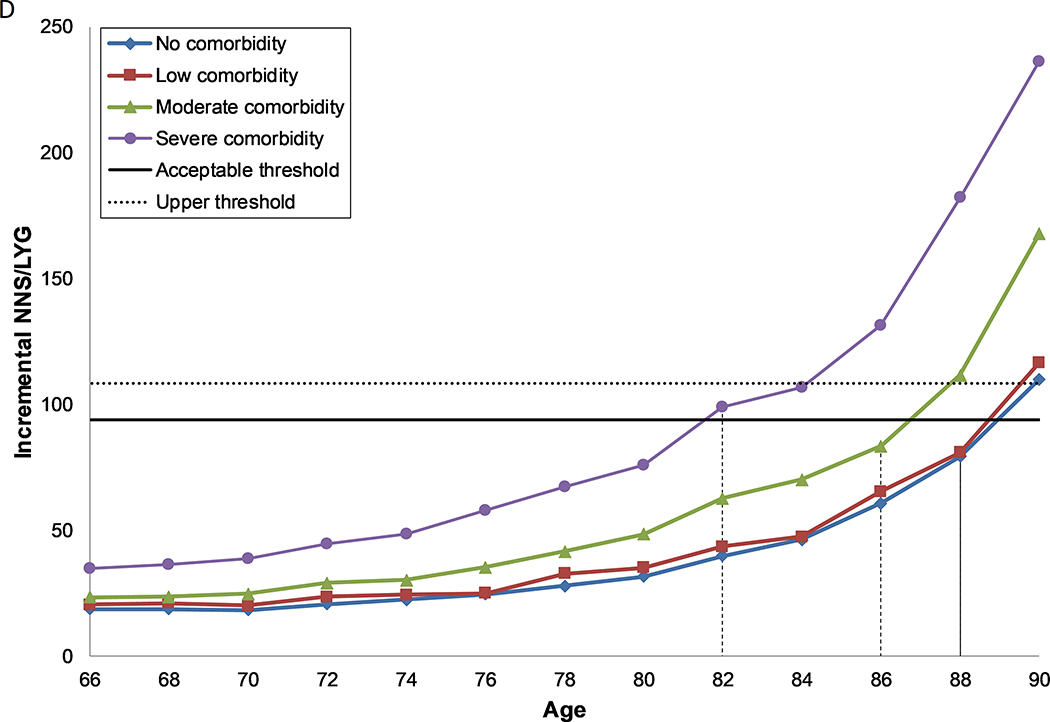
Results: For persons age 76 years, 157 women and 108 men with a perfect screening history would need to be screened to gain 1 life-year per 1000 screened individuals. Previously unscreened women with no comorbid conditions and no history of screening could undergo an initial screening through 90 years, whereas unscreened men could undergo initial screening through 88 years, before this balance is reached. As screening adherence improved or as comorbidities increased, the optimal age to stop screening decreased to a point that, regardless of sex, individuals with severe comorbidities and a perfect screening history should stop screening at age 66 years or younger.
Conclusions: Based on the harm-benefit balance, the optimal stop age for colorectal cancer screening ranges from 66 years for unhealthy individuals with a perfect screening history to 90 years for healthy individuals without prior screening. These findings can be used to assist patients and clinicians in making decisions about screening participation.
Keywords: Colon Cancer; Detection; Patient Outcomes; Precision Medicine.
Copyright © 2021 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Screening History and Comorbidities Help Refine Stop Ages for Colorectal Cancer Screening.Clin Gastroenterol Hepatol. 2021 Mar;19(3):448-450. doi: 10.1016/j.cgh.2020.07.028. Epub 2020 Jul 18. Clin Gastroenterol Hepatol. 2021. PMID: 32693048 Free PMC article. No abstract available.
References
-
- Schreuders EH, Ruco A, Rabeneck L, et al. Colorectal cancer screening: a global overview of existing programmes. Gut 2015;64:1637–49. - PubMed
-
- U.S. Preventive Services Task Force, Bibbins-Domingo K, Grossman DC, et al. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2016;315:2564–75. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
