

Estrogen and thrombosis: A bench to bedside review
- PMID: 32450447
- PMCID: PMC7341440
- DOI: 10.1016/j.thromres.2020.05.008
Estrogen and thrombosis: A bench to bedside review
Abstract
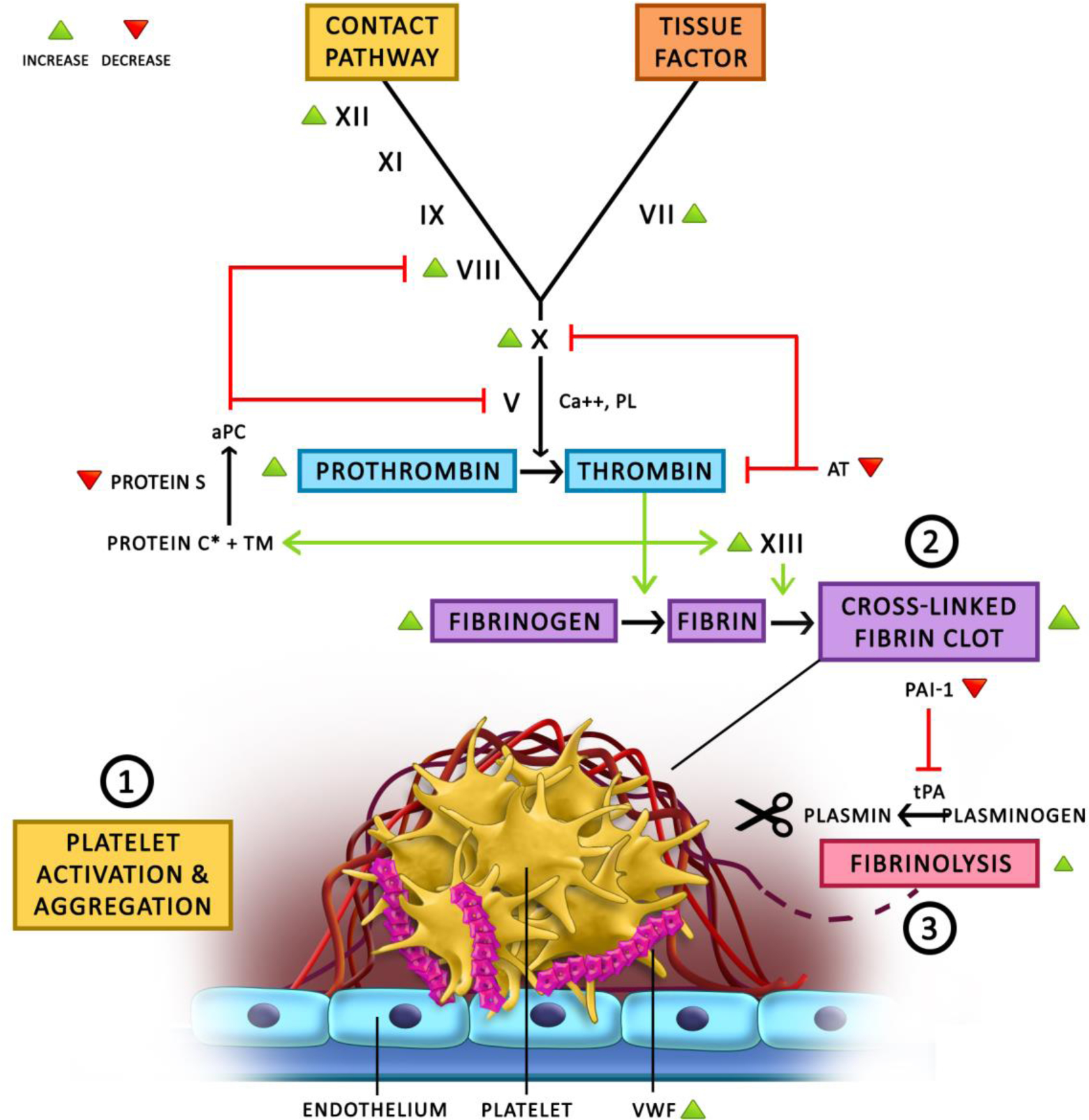
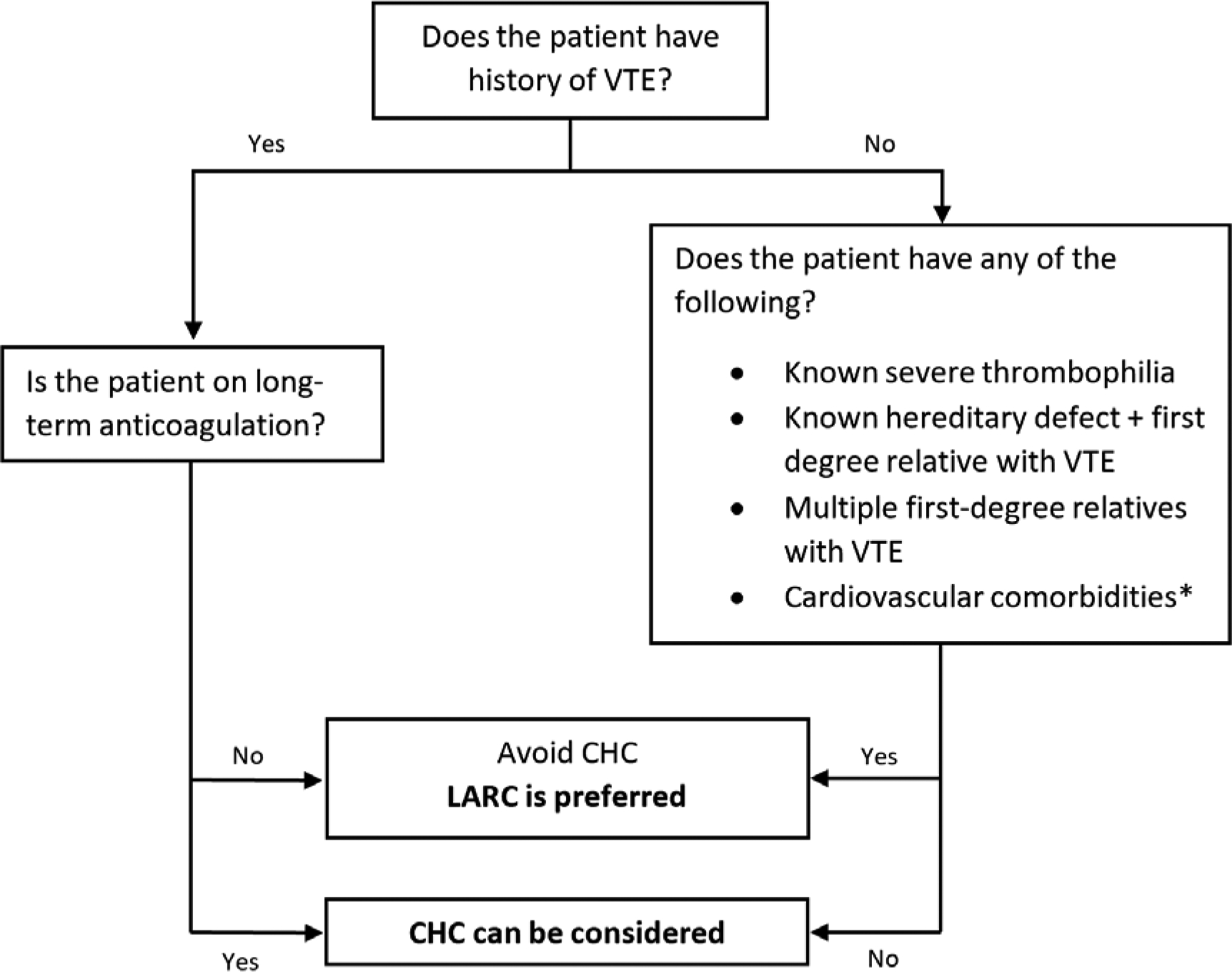
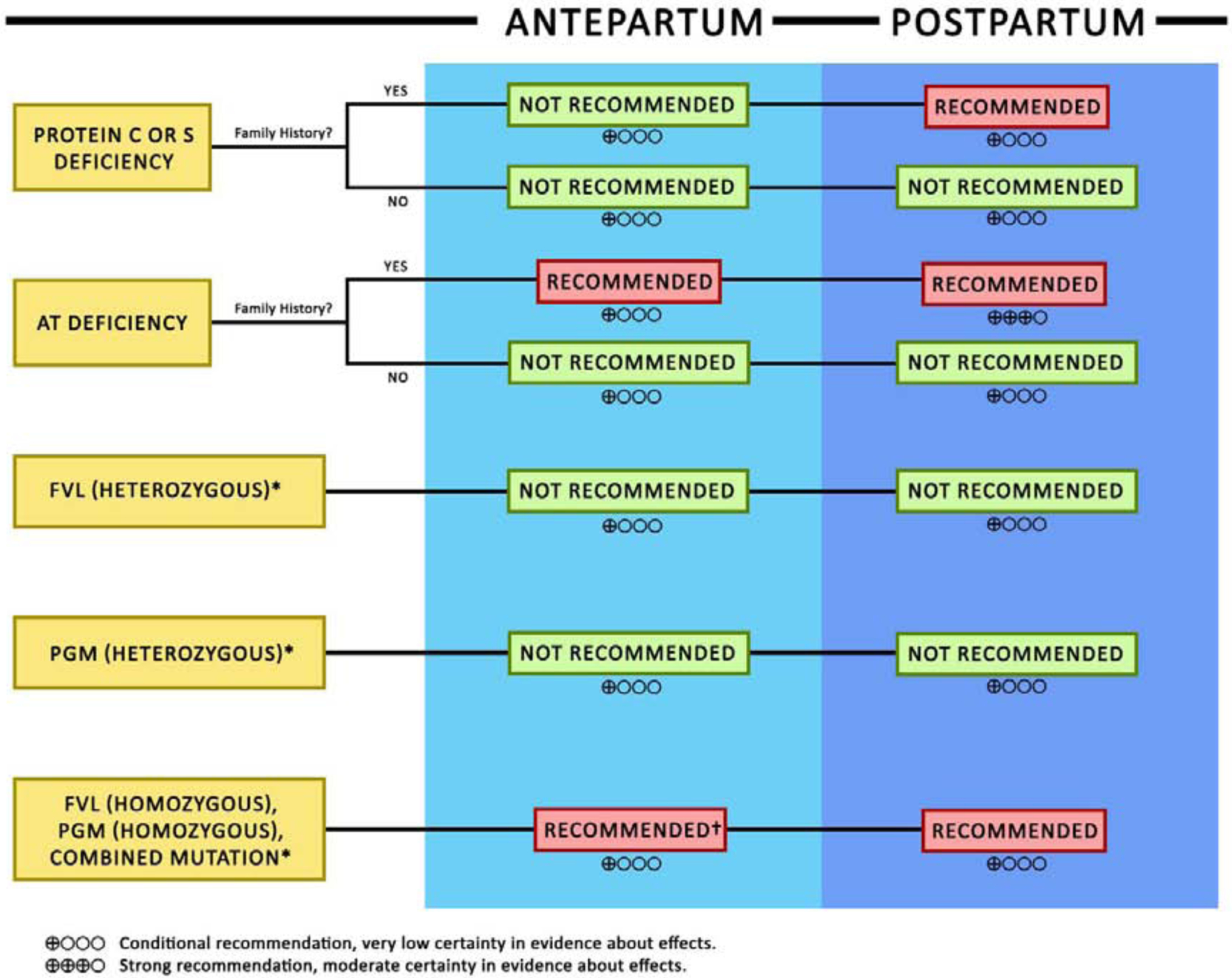
Estrogen, in the clinical setting is used primarily for contraception and hormone replacement therapy. It has been well established that estrogen increases the risk of both arterial and venous thrombosis. While estrogen is known to induce a prothrombotic milieu through various effects on the hemostatic pathways, the exact molecular mechanism leading to those effects is not known. The most common clinical presentation of estrogen-related thrombosis is venous thromboembolism (VTE) of the deep veins of the legs or pulmonary vessels, usually within the first few months of use. Estrogen has also been associated with increased risk of "unusual site" thromboses, as well as arterial thrombosis. Women at high-risk of thrombosis need careful evaluation and counseling for contraception, pregnancy, menopausal hormonal therapy and other estrogen-related conditions or treatments in order to lower the risk of thromboses. We review the most recent evidence on management of high-estrogen states in women at high-risk of thrombosis, as well as emerging data on unique populations such as transgender women. More studies are needed to better understand the pathophysiology of hormone-related thrombosis, as well as more comprehensive techniques to stratify risks for thrombosis so as to enable tailoring of recommendations for each individual.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Letter to the Editors-in-Chief in response to the article of Abou-Ismail, et al. entitled "Estrogen and thrombosis: A bench to bedside review" (Thrombosis Research 192 (2020) 40-51).Thromb Res. 2020 Sep;193:221-223. doi: 10.1016/j.thromres.2020.08.006. Epub 2020 Aug 5. Thromb Res. 2020. PMID: 32798963 No abstract available.
References
-
- Watkins ES, The estrogen elixir: a history of hormone replacement therapy in America. 2007: JHU Press.
-
- Allen E, et al. , The hormone of the ovarian follicle; its localization and action in test animals, and additional points bearing upon the internal secretion of the ovary. American Journal of Anatomy, 1924. 34(1): p. 133–181.
-
- Doisy EA, Veler C, and Thayer S, Folliculin from urine of pregnant women. American Journal of Physiology, 1929. 90(2): p. 329–330.
-
- Huffman MN, et al. , The isolation of α-dihydrotheelin from human pregnancy urine. Journal of Biological Chemistry, 1940. 134(2): p. 591–604.
-
- Butenandt A, Über „Progynon “ein krystallisiertes weibliches Sexualhormon. Naturwissenschaften, 1929. 17(45): p. 879–879.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
