

High prevalence of symptomatic spinal stenosis in Norwegian adults with achondroplasia: a population-based study
- PMID: 32450891
- PMCID: PMC7249360
- DOI: 10.1186/s13023-020-01397-6
High prevalence of symptomatic spinal stenosis in Norwegian adults with achondroplasia: a population-based study
Erratum in
-
Correction to: High prevalence of symptomatic spinal stenosis in Norwegian adults with achondroplasia: a population-based study.Orphanet J Rare Dis. 2020 Dec 7;15(1):342. doi: 10.1186/s13023-020-01636-w. Orphanet J Rare Dis. 2020. PMID: 33287852 Free PMC article.
Abstract
Background: Symptomatic spinal stenosis (SSS) is a well-known medical complication in achondroplasia. The reported prevalence of SSS is 10 to 30%, an estimate based on small studies or selected populations. No population-based studies exist currently. Furthermore, the relationship between SSS and physical functioning has not been investigated in detail. The aims of this study were to describe the prevalence of SSS in Norwegian adults with achondroplasia, and to explore the impact of SSS on physical functioning.
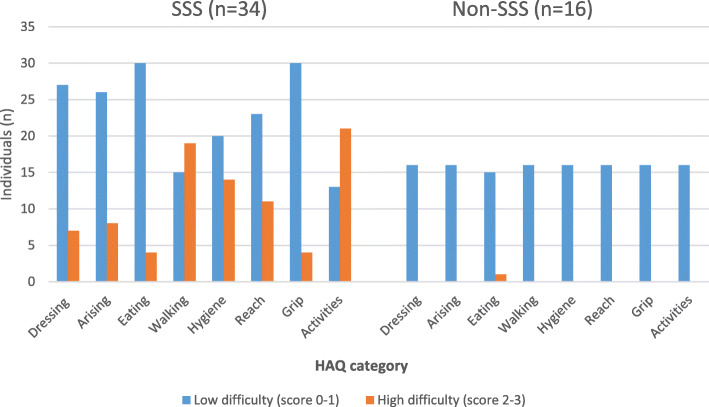
Methods: This was a population-based study on Norwegian community-dwelling adults with genetically confirmed achondroplasia. Prevalence of SSS was defined by clinical symptoms, and confirmed by imaging or surgical reports. Physical functioning was assessed by walking capacity (6-min walk test), hand strength (Grippit), and activities of daily living (the Health Assessment Questionnaire, HAQ). Pain was assessed by pain site locations and intensity (Numeric Rating Scale, NRS).
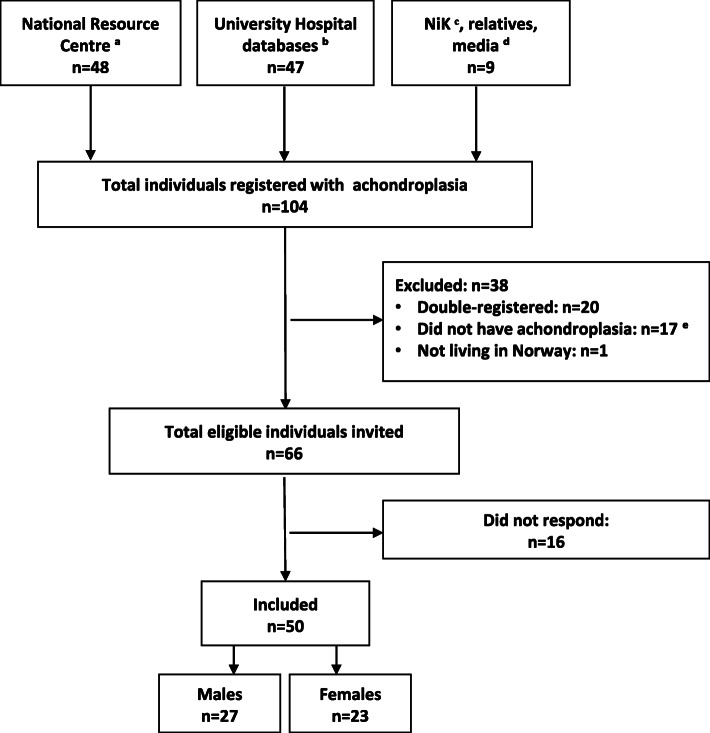
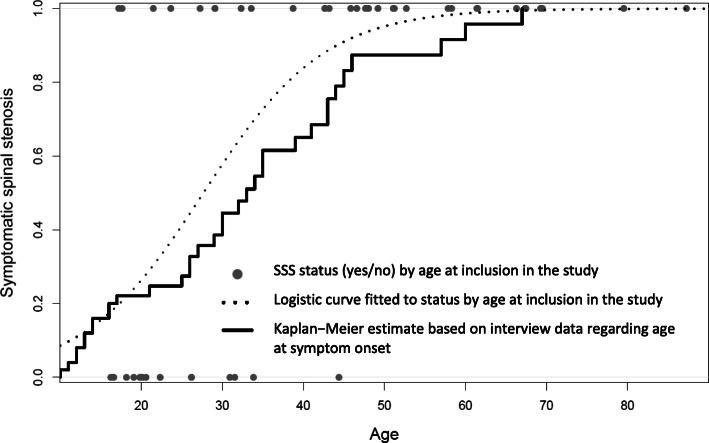
Results: In total, 50 participants were included (27 males, 23 females). Median age was 41 years (range 16 to 87 years), 34 (68%) had SSS. The estimated median age at first symptom onset was 33 years (95% confidence interval (CI) 29 to 43 years), range 10 to 67 years. The majority had multiple spinal levels affected. The walking distance was 110 m shorter in the SSS group (95% CI - 172 to - 40 m) as compared with the non-SSS group (p < 0.01). There was no considerable difference in hand strength between the two groups. Mean HAQ scores (0-3) for walking and hygiene were significantly higher in the SSS group, reflecting more activity limitations. Mean differences were 0.9 (95% CI 0.3 to 1.4, p < 0.01) and 0.6 (95% CI 0.2 to 1.0, p < 0.01). Pain intensity (NRS 0-10) was also significantly higher in the SSS group with a mean difference of 3.2 (95% CI 0.6 to 5.6, p = 0.02).
Conclusions: SSS was highly prevalent in Norwegian adults with achondroplasia, with symptom onset at young age, and multiple spinal levels affected. The presence of SSS was associated with reduced walking distance, activity limitations, and more pain. The findings underline the importance of thorough assessment and monitoring of SSS in achondroplasia, including a formal assessment of physical functioning.
Keywords: 6-minute walk test; Achondroplasia; Activities of daily living; Adults; Hand strength; Pain; Spinal stenosis.
Conflict of interest statement
SOF has received a consulting fee from BioMarin. The authors have completed the ICMJE form and have declared no conflict of interest.
Figures
References
-
- Carlisle ES, Ting BL, Abdullah MA, Skolasky RL, Schkrohowsky JG, Yost MT, et al. Laminectomy in patients with achondroplasia: the impact of time to surgery on long-term function. Spine. 2011;36(11):886–892. - PubMed
-
- Schkrohowsky JG, Hoernschemeyer DG, Carson BS, Ain MC. Early presentation of spinal stenosis in achondroplasia. J Pediatr Orthop. 2007;27(2):119–122. - PubMed
-
- Kreiner DS, Shaffer WO, Baisden JL, Gilbert TJ, Summers JT, Toton JF, et al. An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spinal stenosis (update) Spine J. 2013;13(7):734–743. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
