

Diagnostic and prognostic values of the QRS-T angle in patients with suspected acute decompensated heart failure
- PMID: 32452635
- PMCID: PMC7373892
- DOI: 10.1002/ehf2.12746
Diagnostic and prognostic values of the QRS-T angle in patients with suspected acute decompensated heart failure
Abstract
Aims: The aim of this study was to investigate the diagnostic and prognostic utility of the QRS-T angle, an electrocardiogram (ECG) marker quantifying depolarization-repolarization heterogeneity, in patients with suspected acute decompensated heart failure (ADHF).
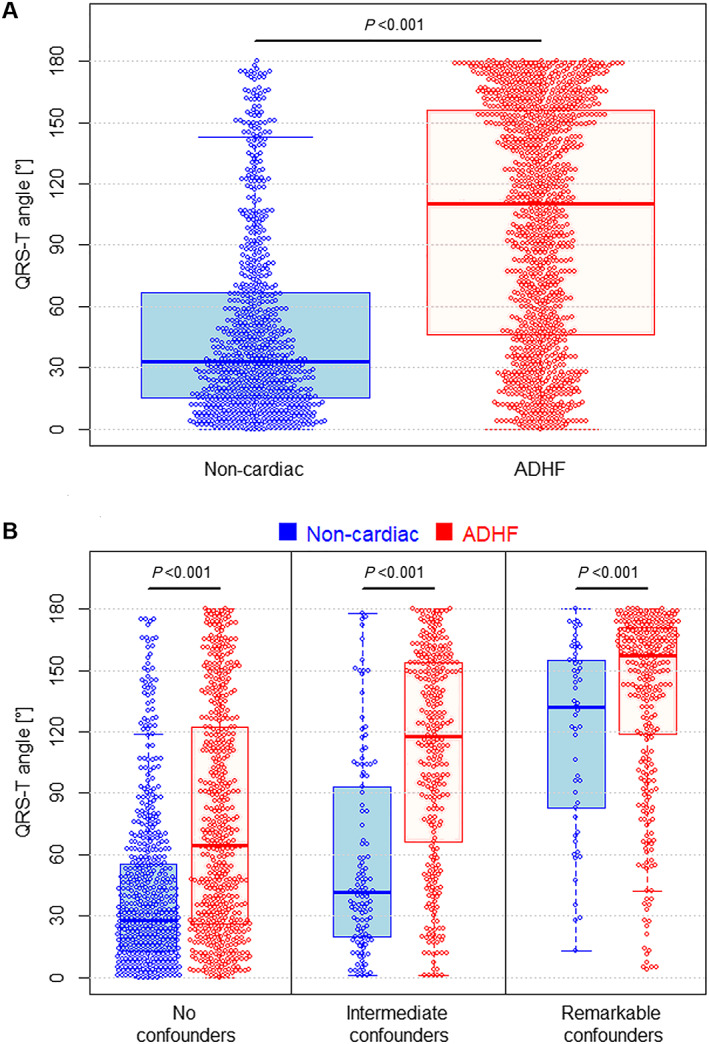
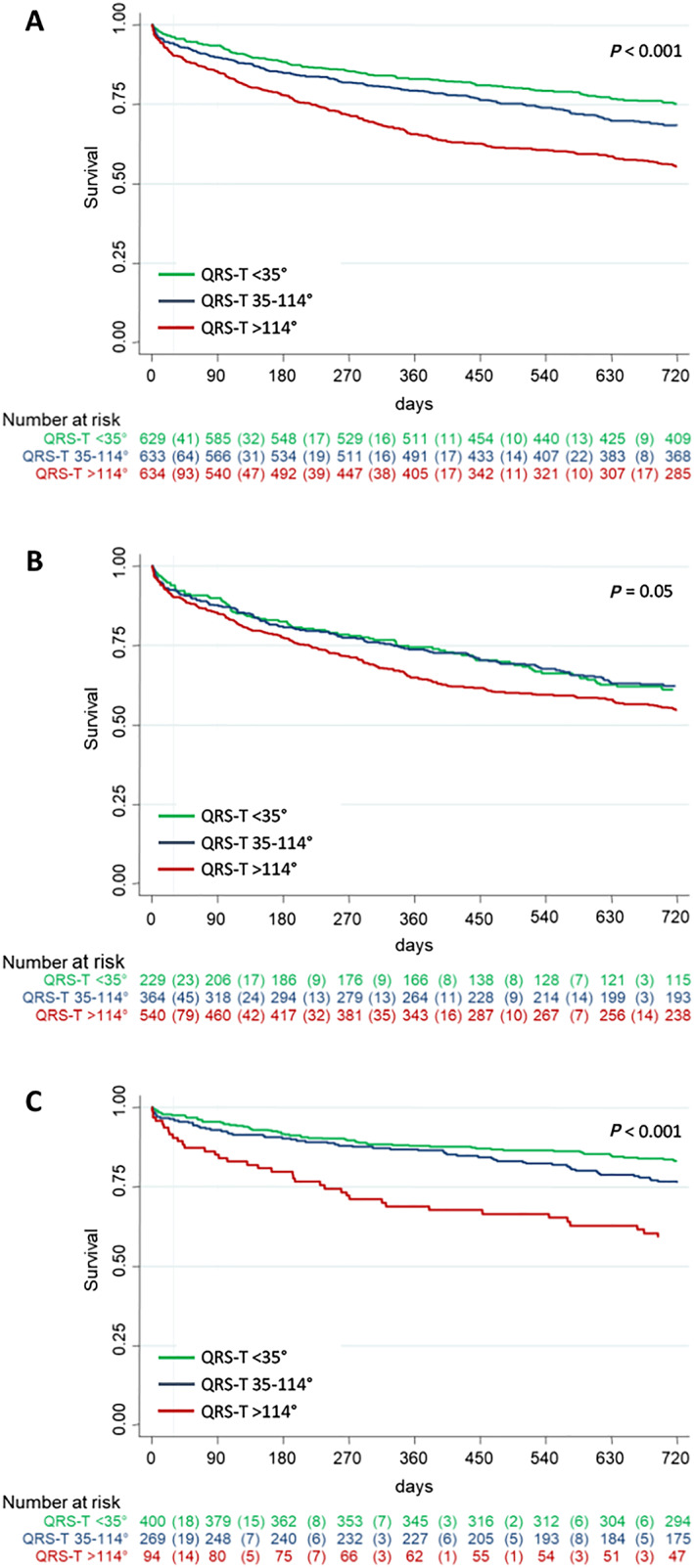
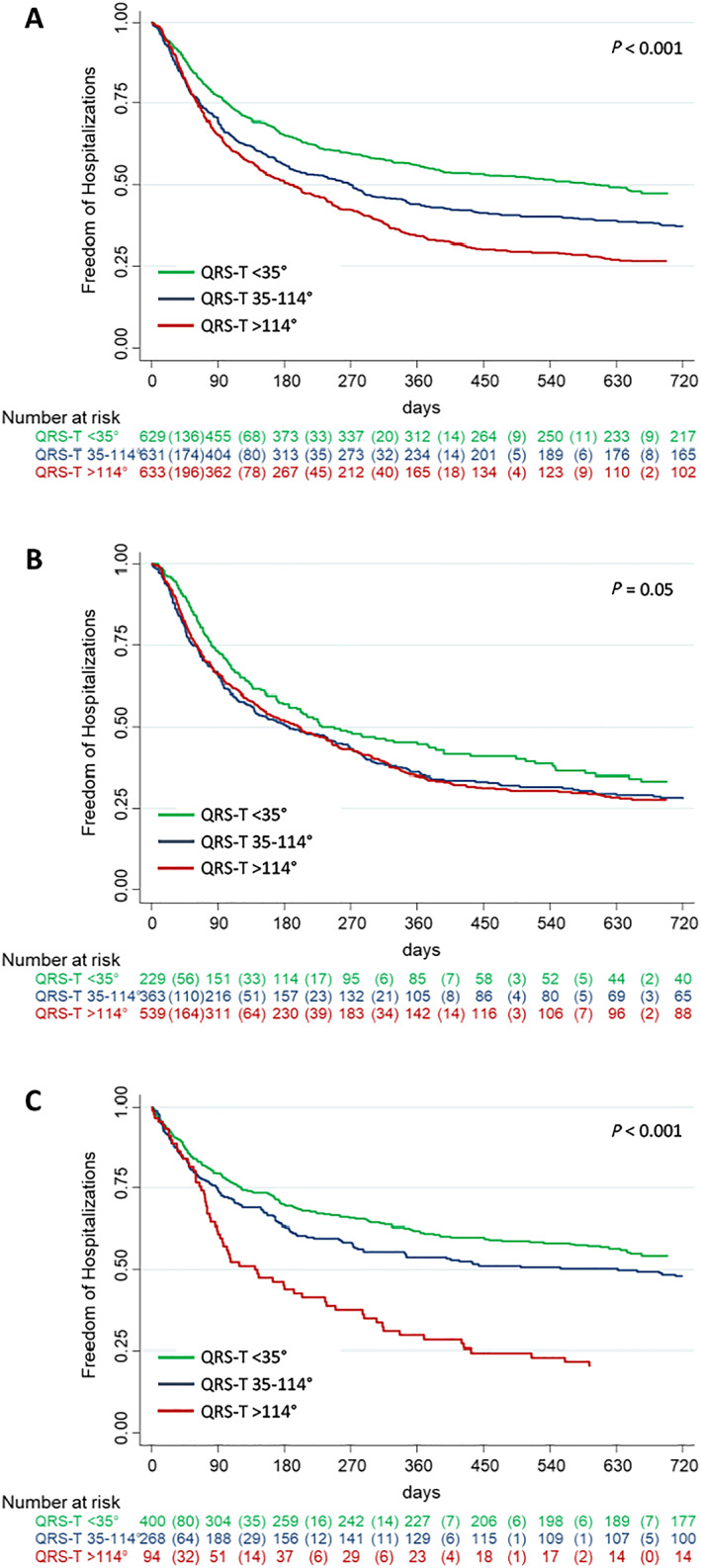
Methods and results: We prospectively enrolled unselected patients presenting to the emergency department with symptoms suggestive of ADHF. The QRS-T angle was automatically derived from a standard 12-lead ECG recorded at presentation. The primary diagnostic endpoint was a final adjudicated diagnosis of ADHF. The primary prognostic endpoint was all-cause mortality during 2 years of follow-up. Among the 1915 patients enrolled, those with higher QRS-T angles were older, were more commonly male, and had a higher rate of co-morbidities such as arterial hypertension, coronary artery disease, or chronic kidney disease. ADHF was the final adjudicated diagnosis in 1140 (60%) patients. The QRS-T angle in patients with ADHF was significantly larger than in patients with non-cardiac causes of dyspnoea {median 110° [inter-quartile range (IQR) 46-156°] vs. median 33° [IQR 15-57°], P < 0.001}. The diagnostic accuracy of the QRS-T angle as quantified by the area under the receiver operating characteristic curve (AUC) was 0.75 [95% confidence interval (CI) 0.73-0.77, P < 0.001], which was inferior to N-terminal pro-B-type natriuretic peptide (AUC 0.93, 95% CI 0.92-0.94, P < 0.001), but similar to that of high-sensitivity troponin T (AUC 0.78, 95% CI 0.76-0.80, P = 0.09). The AUC of the QRS-T angle for discrimination between ADHF and non-cardiac dyspnoea remained similarly high in subgroups of patients known to be diagnostically challenging, including patients older than 75 years [0.71 (95% CI 0.67-0.74)], renal failure [0.79 (95% CI 0.71-0.87)], and atrial fibrillation at presentation [0.68 (95% CI 0.60-0.76)]. Mortality rates according to QRS-T angle tertiles were 4%, 6%, and 10% after 30 days (P < 0.001) and 24%, 31%, and 43% after 2 years (P < 0.001). After adjustment for clinical, laboratory, and ECG parameters, the QRS-T angle remained an independent predictor for 2 year mortality with a 4% increase in mortality for every 20° increase in QRS-T angle (P = 0.02).
Conclusions: The QRS-T angle is a readily available and inexpensive marker that can assist in the discrimination between ADHF and non-cardiac causes of acute dyspnoea and may aid in the risk stratification of these patients.
Keywords: Acute dyspnoea; Acute heart failure; ECG; Heart failure; QRS-T angle.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
T.B. has received research grants from the Swiss National Science Foundation (PASMP3‐134362), the Department of Internal Medicine, University Hospital Basel, Abbott, and Roche as well as speaker honoraria from Roche. C.M. has received research grants from the Swiss National Science Foundation, the Swiss Heart Foundation, the European Union, the Cardiovascular Research Foundation Basel, the KTI, the University of Basel, Abbott, Alere, AstraZeneca, Beckman Coulter, BG Medicine, Biomerieux, BRAHMS, Critical Diagnostics, Roche, Siemens, Singulex, Sphingotec, and 8sense as well as speaker/consulting honoraria from Abbott, Alere, AstraZeneca, Biomerieux, BMS, Boehringer Ingelheim, BRAHMS, Cardiorentis, Eli Lilly, Novartis, Roche, Sanofi, Siemens, and Singulex. T.R. has received research grants from the Goldschmidt‐Jacobson Foundation, the Swiss National Science Foundation, the Swiss Heart Foundation, the European Union (Eurostars 9799—ALVALE), the Professor Max Cloëtta Foundation, the Cardiovascular Research Foundation Basel, the University of Basel, and the University Hospital Basel, all for work outside the submitted study. He has received speaker/consulting honoraria or travel support from Abbott/SJM, Astra Zeneca, Brahms, Bayer, Biosense‐Webster, Biotronik, Boston‐Scientific, Daiichi Sankyo, Medtronic, Pfizer‐BMS, and Roche, all for work outside the submitted study. He has received support for his institution's fellowship programme from Abbott/SJM, Biosense‐Webster, Biotronik, Boston‐Scientific, and Medtronic for work outside the submitted study. All other authors declare no conflict of interest.
Figures
References
-
- Ambrosy AP, Fonarow GC, Butler J, Chioncel O, Greene SJ, Vaduganathan M, Nodari S, Lam CSP, Sato N, Shah AN, Gheorghiade M. The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J Am Coll Cardiol 2014; 63: 1123–1133. - PubMed
-
- Pang PS, Collins SP, Miró Ò, Bueno H, Diercks DB, Di Somma S, Gray A, Harjola V‐P, Hollander JE, Lambrinou E, Levy PD, Papa A, Möckel M. Editor's choice—the role of the emergency department in the management of acute heart failure: an international perspective on education and research. Eur Heart J Acute Cardiovasc Care 2017; 6: 421–429. - PubMed
-
- Gouda P, Brown P, Rowe BH, McAlister FA, Ezekowitz JA. Insights into the importance of the electrocardiogram in patients with acute heart failure. Eur J Heart Fail 2016; 18: 1032–1040. - PubMed
-
- Pavri BB, Hillis MB, Subačius H, Brumberg GE, Schaechter A, Levine JH, Kadish A. Prognostic value and temporal behavior of the planar QRS‐T angle in patients with nonischemic cardiomyopathy. Circulation 2008; 117: 3181–3186. - PubMed
-
- Borleffs CJW, Scherptong RWC, Man S‐C, van Welsenes GH, Bax JJ, van Erven L, Swenne CA, Schalij MJ. Predicting ventricular arrhythmias in patients with ischemic heart disease. Circ Arrhythmia Electrophysiol. 2009; 2: 548–554. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
