

Safety, Tolerability, and Efficacy of Viltolarsen in Boys With Duchenne Muscular Dystrophy Amenable to Exon 53 Skipping: A Phase 2 Randomized Clinical Trial
- PMID: 32453377
- PMCID: PMC7251505
- DOI: 10.1001/jamaneurol.2020.1264
Safety, Tolerability, and Efficacy of Viltolarsen in Boys With Duchenne Muscular Dystrophy Amenable to Exon 53 Skipping: A Phase 2 Randomized Clinical Trial
Erratum in
-
Error in Figure.JAMA Neurol. 2020 Aug 1;77(8):1040. doi: 10.1001/jamaneurol.2020.2025. JAMA Neurol. 2020. PMID: 32539096 Free PMC article. No abstract available.
Abstract
Importance: An unmet need remains for safe and efficacious treatments for Duchenne muscular dystrophy (DMD). To date, there are limited agents available that address the underlying cause of the disease.
Objective: To evaluate the safety, tolerability, and efficacy of viltolarsen, a novel antisense oligonucleotide, in participants with DMD amenable to exon 53 skipping.
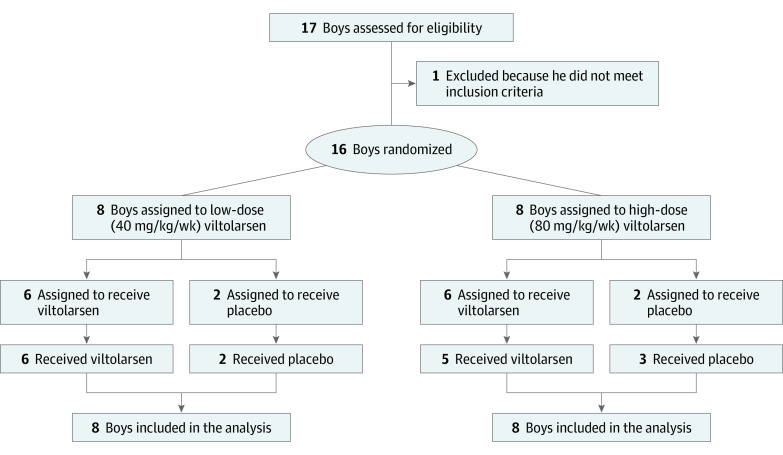
Design, setting, and participants: This phase 2 study was a 4-week randomized clinical trial for safety followed by a 20-week open-label treatment period of patients aged 4 to 9 years with DMD amenable to exon 53 skipping. To enroll 16 participants, with 8 participants in each of the 2 dose cohorts, 17 participants were screened. Study enrollment occurred between December 16, 2016, and August 17, 2017, at sites in the US and Canada. Data were collected from December 2016 to February 2018, and data were analyzed from April 2018 to May 2019.
Interventions: Participants received 40 mg/kg (low dose) or 80 mg/kg (high dose) of viltolarsen administered by weekly intravenous infusion.
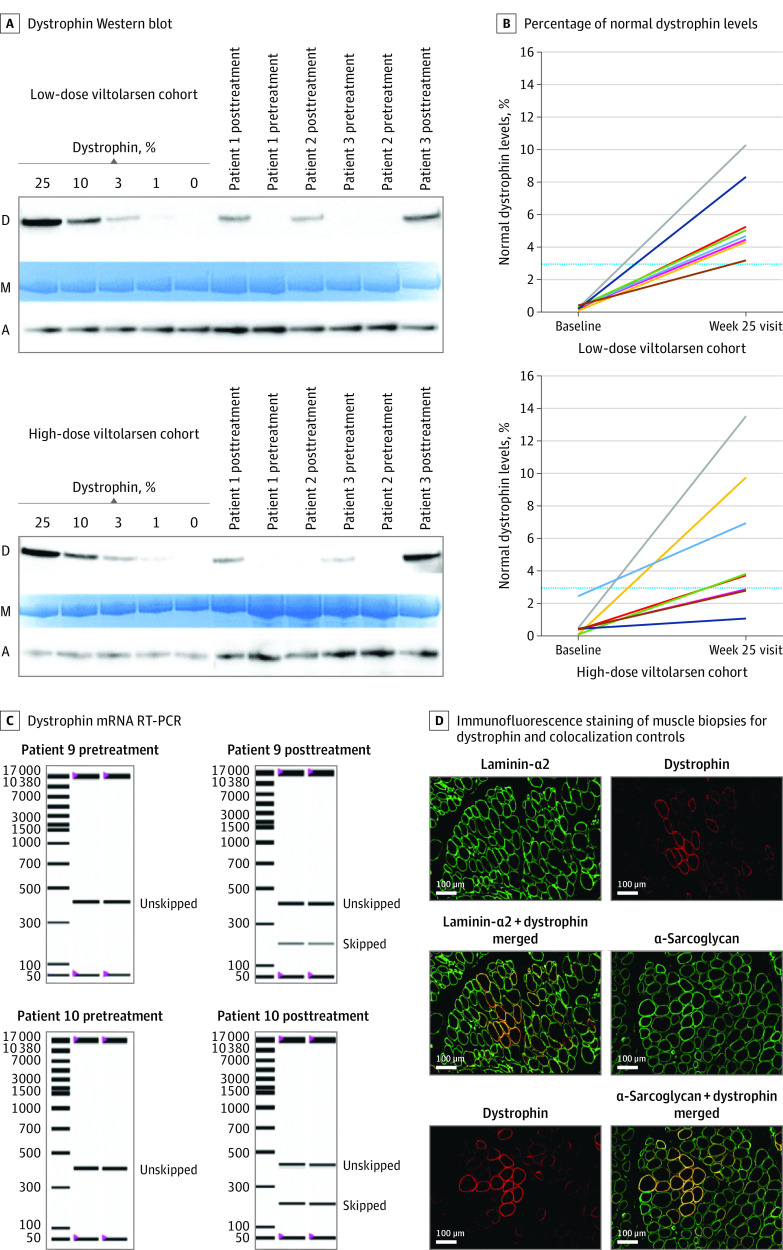
Main outcomes and measures: Primary outcomes of the trial included safety, tolerability, and de novo dystrophin protein production measured by Western blot in participants' biceps muscles. Secondary outcomes included additional assessments of dystrophin mRNA and protein production as well as clinical muscle strength and function.
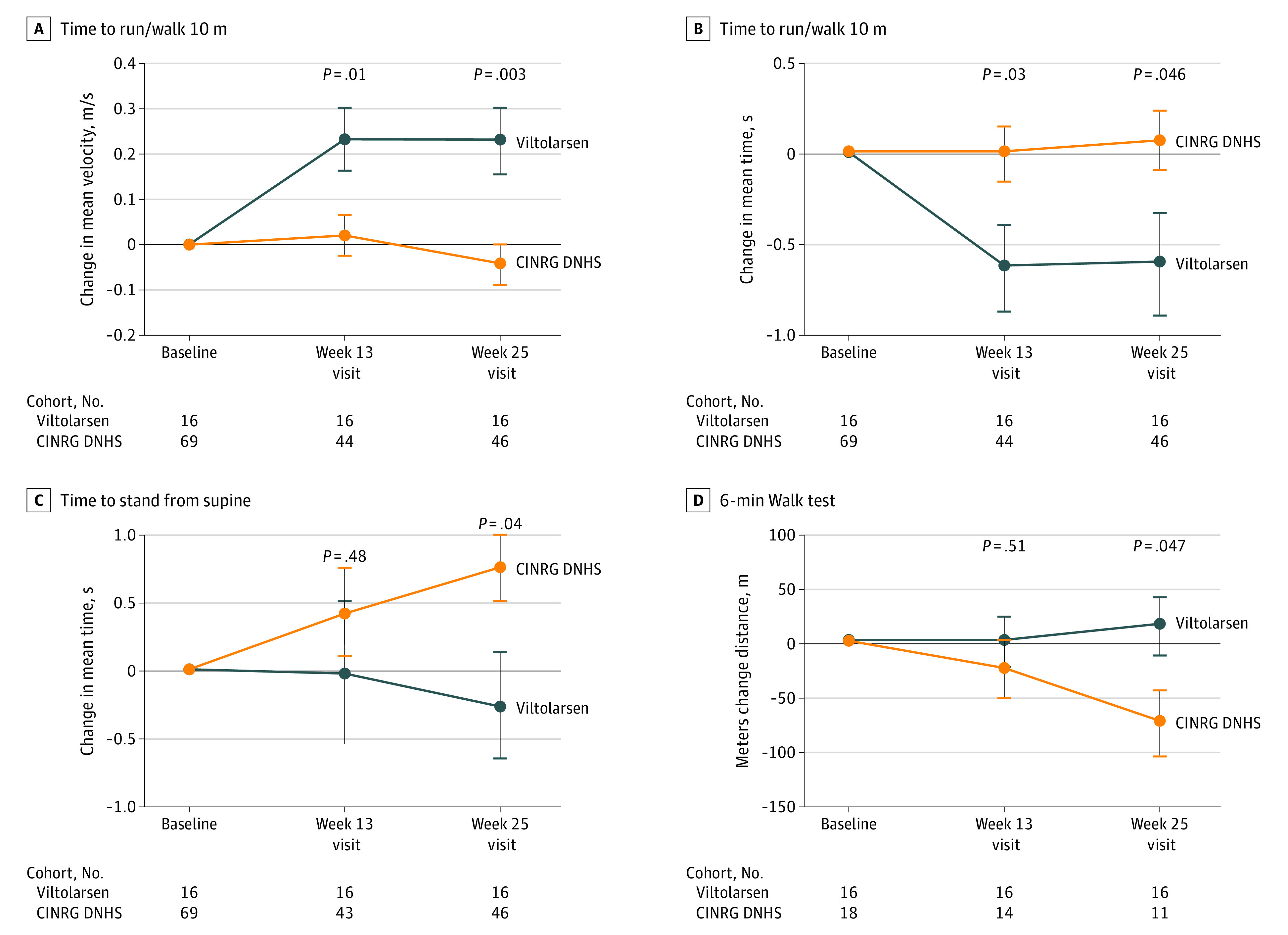
Results: Of the 16 included boys with DMD, 15 (94%) were white, and the mean (SD) age was 7.4 (1.8) years. After 20 to 24 weeks of treatment, significant drug-induced dystrophin production was seen in both viltolarsen dose cohorts (40 mg/kg per week: mean [range] 5.7% [3.2-10.3] of normal; 80 mg/kg per week: mean [range] 5.9% [1.1-14.4] of normal). Viltolarsen was well tolerated; no treatment-emergent adverse events required dose reduction, interruption, or discontinuation of the study drug. No serious adverse events or deaths occurred during the study. Compared with 65 age-matched and treatment-matched natural history controls, all 16 participants treated with viltolarsen showed significant improvements in timed function tests from baseline, including time to stand from supine (viltolarsen: -0.19 s; control: 0.66 s), time to run/walk 10 m (viltolarsen: 0.23 m/s; control: -0.04 m/s), and 6-minute walk test (viltolarsen: 28.9 m; control: -65.3 m) at the week 25 visit.
Conclusions and relevance: Systemic treatment of participants with DMD with viltolarsen induced de novo dystrophin production, and clinical improvement of timed function tests was observed.
Trial registration: ClinicalTrials.gov Identifier: NCT02740972.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
