

Assessment of Racial and Ethnic Disparities in the Use of Medication to Treat Opioid Use Disorder Among Pregnant Women in Massachusetts
- PMID: 32453384
- PMCID: PMC7251447
- DOI: 10.1001/jamanetworkopen.2020.5734
Assessment of Racial and Ethnic Disparities in the Use of Medication to Treat Opioid Use Disorder Among Pregnant Women in Massachusetts
Abstract
Importance: Racial and ethnic disparities persist across key health and substance use treatment outcomes for mothers and infants. The use of medications, such as methadone or buprenorphine, for the treatment of opioid use disorder (OUD) has been associated with improvements in the outcomes of mothers and infants; however, only half of all pregnant women with OUD receive these medications. The extent to which maternal race or ethnicity is associated with the use of medication to treat OUD, the duration of the use of medication to treat OUD, and the type of medication used to treat OUD during pregnancy are unknown.
Objective: To examine the extent to which maternal race and ethnicity is associated with the use of medications for the treatment of OUD in the year before delivery among pregnant women with OUD.
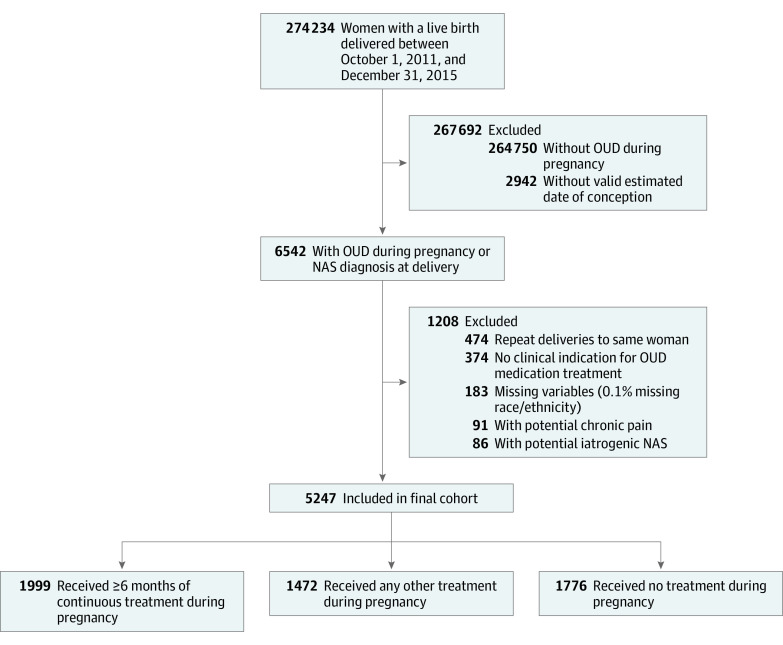
Design, setting, and participants: This retrospective cohort study used a linked population-level statewide data set of pregnant women with OUD who delivered a live infant in Massachusetts between October 1, 2011, and December 31, 2015. Of 274 234 total deliveries identified, 5247 deliveries among women with indicators of having OUD were included in the analysis. Maternal race and ethnicity were defined as white non-Hispanic, black non-Hispanic, or Hispanic based on self-reported data on birth certificates.
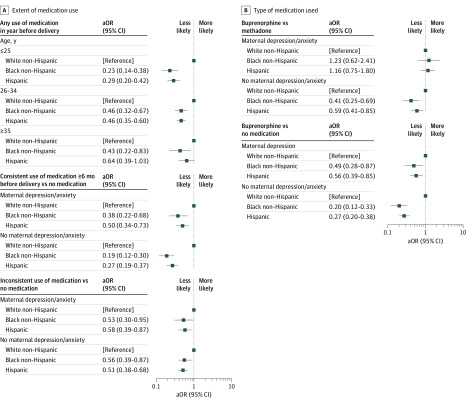
Main outcomes and measures: Main outcomes were the receipt of any medication for OUD, the consistency of the use of medication (at least 6 continuous months of use before delivery, inconsistent use, or no use) for the treatment of OUD, and the type of medication (methadone or buprenorphine) used to treat OUD. Multivariable models were adjusted for maternal sociodemographic characteristics, comorbidities, and any significant interactions between the covariates and race and ethnicity.
Results: The sample included 5247 pregnant women with OUD who delivered a live infant in Massachusetts during the study period. The mean (SD) maternal age at delivery was 28.7 (5.0) years; 4551 women (86.7%) were white non-Hispanic, 462 women (8.8%) were Hispanic, and 234 women (4.5%) were black non-Hispanic. A total of 3181 white non-Hispanic women (69.9%) received any type of medication for the treatment of OUD in the year before delivery compared with 228 Hispanic women (49.4%) and 108 black non-Hispanic women (46.2%). Compared with white non-Hispanic women, black non-Hispanic and Hispanic women had a substantially lower likelihood (adjusted odds ratio [aOR], 0.37; 95% CI, 0.28-0.49 and aOR, 0.42; 95% CI, 0.35-0.52, respectively) of receiving any medication for the treatment of OUD. Stratification by maternal age identified greater disparities among younger women. Black non-Hispanic and Hispanic women also had a lower likelihood (aOR, 0.24; 95% CI, 0.17-0.35 and aOR, 0.34; 95% CI, 0.27-0.44, respectively) of consistent use of medication for the treatment of OUD compared with white non-Hispanic women. With respect to the type of medication used to treat OUD, black non-Hispanic and Hispanic women had a lower likelihood (aOR, 0.60; 95% CI, 0.40-0.90 and aOR, 0.77; 95% CI, 0.58-1.01, respectively) than white non-Hispanic women of receiving buprenorphine treatment compared with methadone treatment.
Conclusions and relevance: This study found racial and ethnic disparities in the use of medications to treat OUD during pregnancy, with black non-Hispanic and Hispanic women significantly less likely to use medications consistently or at all compared with white non-Hispanic women. Further investigation of patient, clinician, treatment program, and system-level factors associated with these findings is warranted.
Conflict of interest statement
Figures
References
-
- Comer S, Cunningham C, Fishman MJ, et al. . The National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use American Society of Addiction Medicine; 2015. Accessed May 26, 2019. https://www.asam.org/docs/default-source/practice-support/guidelines-and...
-
- American Society of Addiction Medicine Public Policy Statement on Substance Use, Misuse, and Use Disorders During and Following Pregnancy, With an Emphasis on Opioids Background American Society of Addiction Medicine; 2017. Accessed May 3, 2018. https://www.asam.org/docs/default-source/public-policy-statements/substa...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
