

Association of Intrauterine Growth Restriction and Small for Gestational Age Status With Childhood Cognitive Outcomes: A Systematic Review and Meta-analysis
- PMID: 32453414
- PMCID: PMC7251506
- DOI: 10.1001/jamapediatrics.2020.1097
Association of Intrauterine Growth Restriction and Small for Gestational Age Status With Childhood Cognitive Outcomes: A Systematic Review and Meta-analysis
Abstract
Importance: The magnitude of the association of intrauterine growth restriction (IUGR) and small for gestational age (SGA) status with cognitive outcomes in preterm and term-born children has not been established.
Objective: To examine cognitive outcomes of preterm and term-born children who had IUGR and were SGA compared with children who were appropriate for gestational age (AGA) during the first 12 years of life.
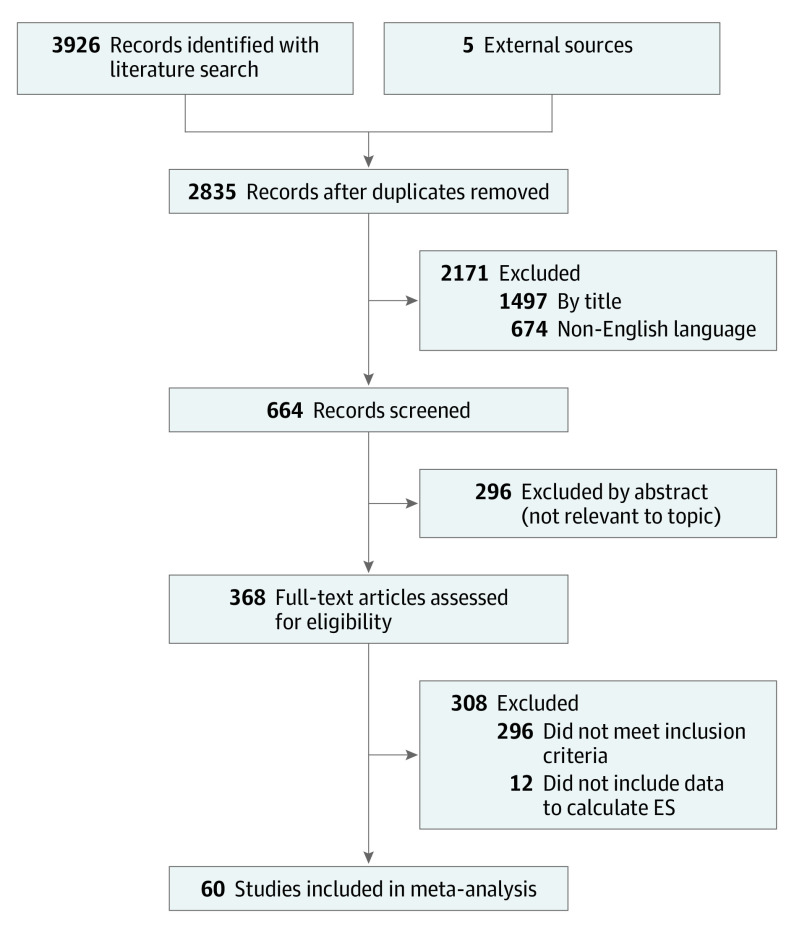
Data sources: For this systematic review and meta-analysis, the Scopus, PubMed, Web of Science, Science Direct, PsycInfo, and ERIC databases were searched for English-language, peer-reviewed literature published between January 1, 2000, and February 20, 2020. The following Medical Subject Heading terms for IUGR and SGA and cognitive outcomes were used: intrauterine growth restriction, intrauterine growth retardation, small for gestational age AND neurodevelopment, neurodevelopmental outcome, developmental outcomes, and cognitive development.
Study selection: Inclusion criteria were assessment of cognitive outcomes (full-scale IQ or a cognitive subscale), inclusion of an AGA group as comparison group, and inclusion of gestational age at birth and completion of cognitive assessment up to 12 years of age.
Data extraction and synthesis: The Meta-analysis of Observational Studies in Epidemiology (MOOSE) reporting guidelines were followed. Data were double screened for full-text articles, and a subset were independently coded by 2 authors. Standardized mean differences (SMDs) and odd ratios from individual studies were pooled by applying random-effects models.
Main outcomes and measures: Cognitive outcomes, defined as mental, cognitive, or IQ scores, estimated with standardized practitioner-based cognitive tests or as borderline intellectual impairment (BII), defined as mental, cognitive, or IQ scores at least 1 SD below the mean cognitive score.
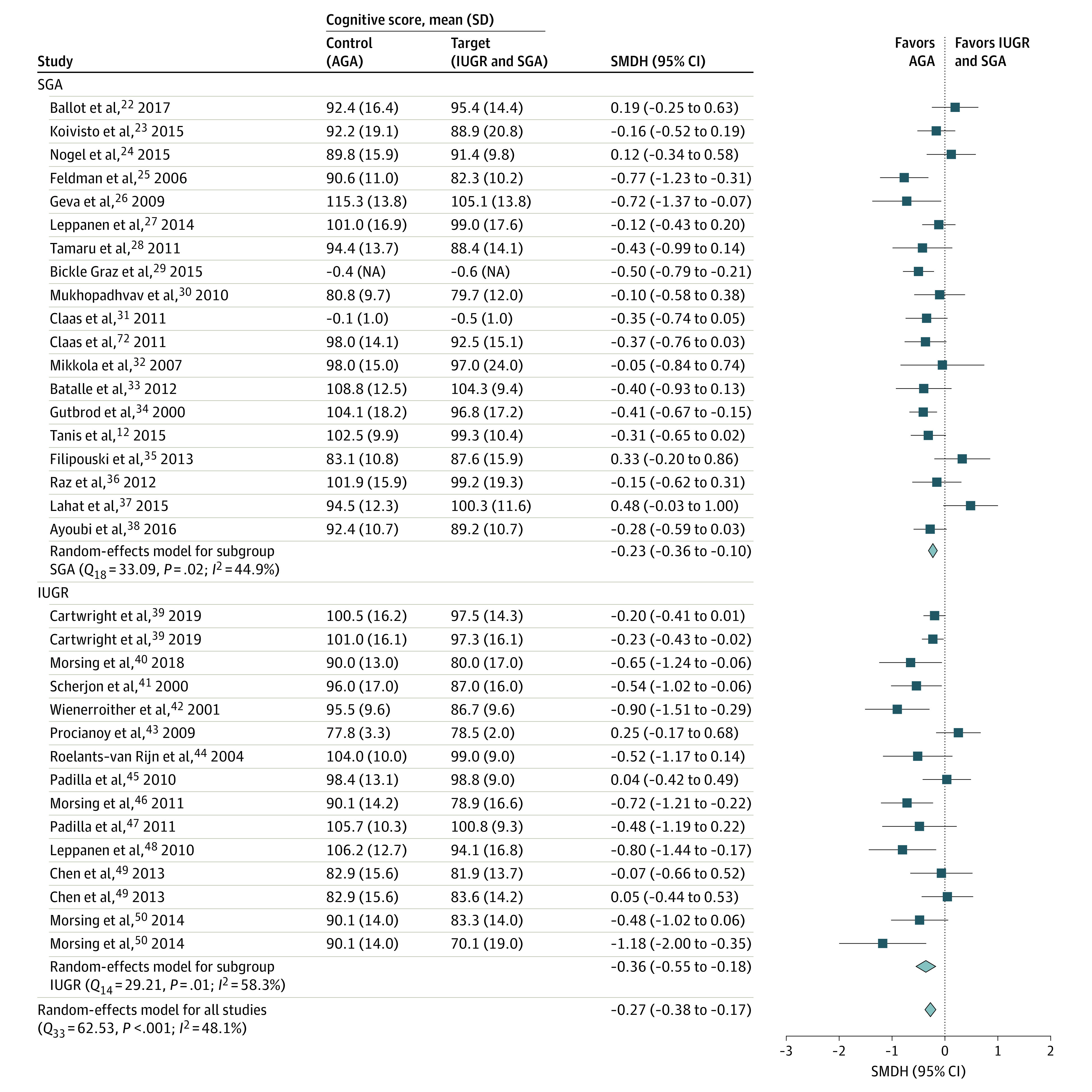
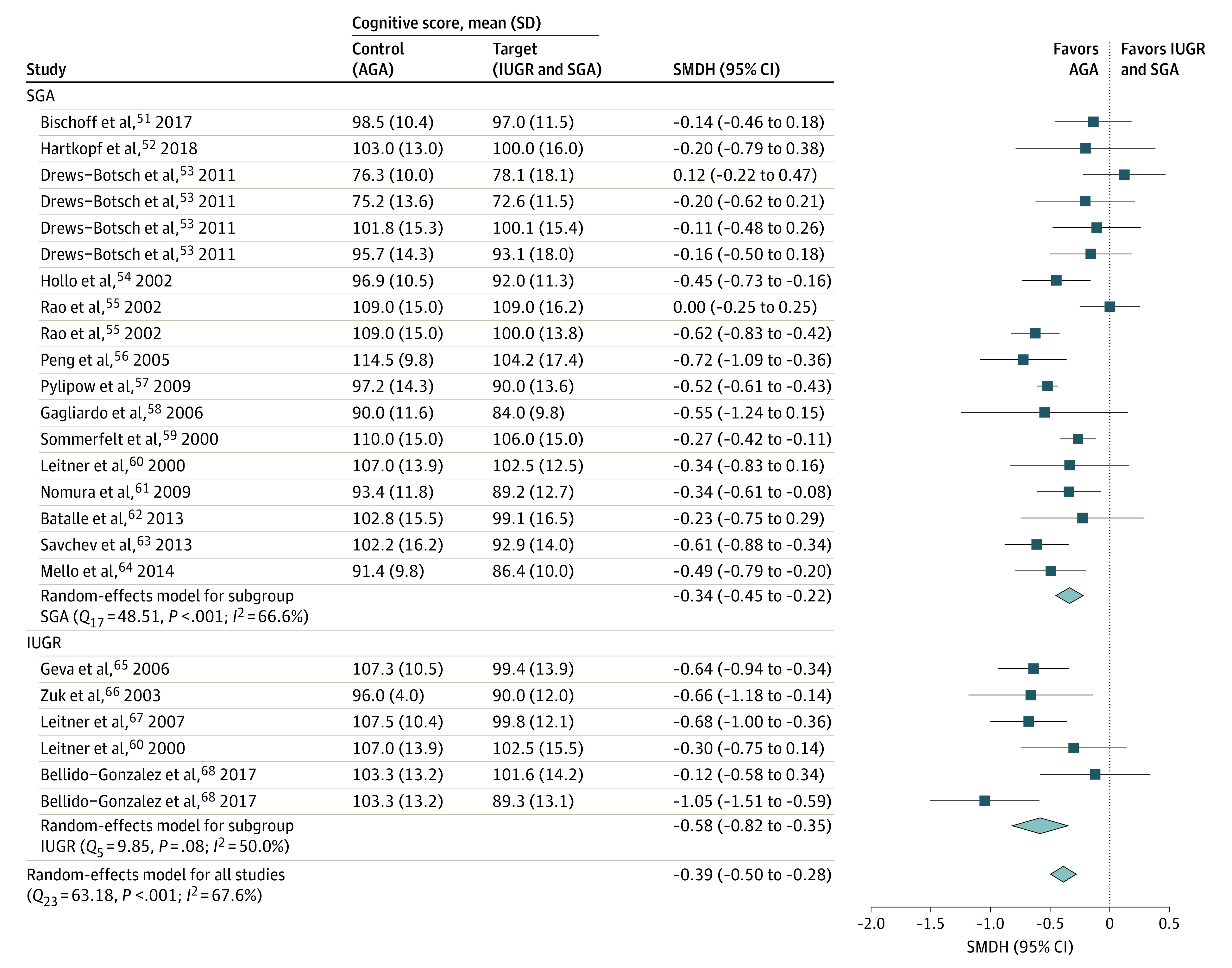
Results: In this study of 89 samples from 60 studies including 52 822 children, children who had IUGR and were SGA had significantly poorer cognitive outcomes (eg, cognitive scores and BII) than children with AGA in childhood. For cognitive scores, associations are consistent for preterm (SMD, -0.27; 95% CI, -0.38 to -0.17) and term-born children (SMD, -0.39; 95% CI, -0.50 to -0.28), with higher effect sizes reported for term-born IUGR and AGA group comparisons (SMD, -0.58; 95% CI, -0.82 to -0.35). Analyses on BII revealed a significantly increased risk in the preterm children who had IUGR and were SGA (odds ratio, 1.57; 95% CI, 1.40-1.77) compared with the children with AGA.
Conclusions and relevance: Growth vulnerabilities assessed antenatally (IUGR) and at the time of birth (SGA) are significantly associated with lower childhood cognitive outcomes in preterm and term-born children compared with children with AGA. These findings highlight the need to develop interventions that boost cognitive functions in these high-risk groups.
Conflict of interest statement
Figures

Comment in
-
Early Detection and Prevention of Intrauterine Growth Restriction and Its Consequences.JAMA Pediatr. 2020 Aug 1;174(8):749-750. doi: 10.1001/jamapediatrics.2020.1106. JAMA Pediatr. 2020. PMID: 32453430 No abstract available.
References
-
- Alkalay AL, Graham JM Jr, Pomerance JJ. Evaluation of neonates born with intrauterine growth retardation: review and practice guidelines. J Perinatol. 1998;18(2):142-151. - PubMed
-
- Lees C, Marlow N, Arabin B, et al. ; TRUFFLE Group . Perinatal morbidity and mortality in early-onset fetal growth restriction: cohort outcomes of the Trial of Randomized Umbilical and Fetal Flow in Europe (TRUFFLE). Ultrasound Obstet Gynecol. 2013;42(4):400-408. doi: 10.1002/uog.13190 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
