

An Integrated Genomic Strategy to Identify CHRNB4 as a Diagnostic/Prognostic Biomarker for Targeted Therapy in Head and Neck Cancer
- PMID: 32455963
- PMCID: PMC7281299
- DOI: 10.3390/cancers12051324
An Integrated Genomic Strategy to Identify CHRNB4 as a Diagnostic/Prognostic Biomarker for Targeted Therapy in Head and Neck Cancer
Abstract
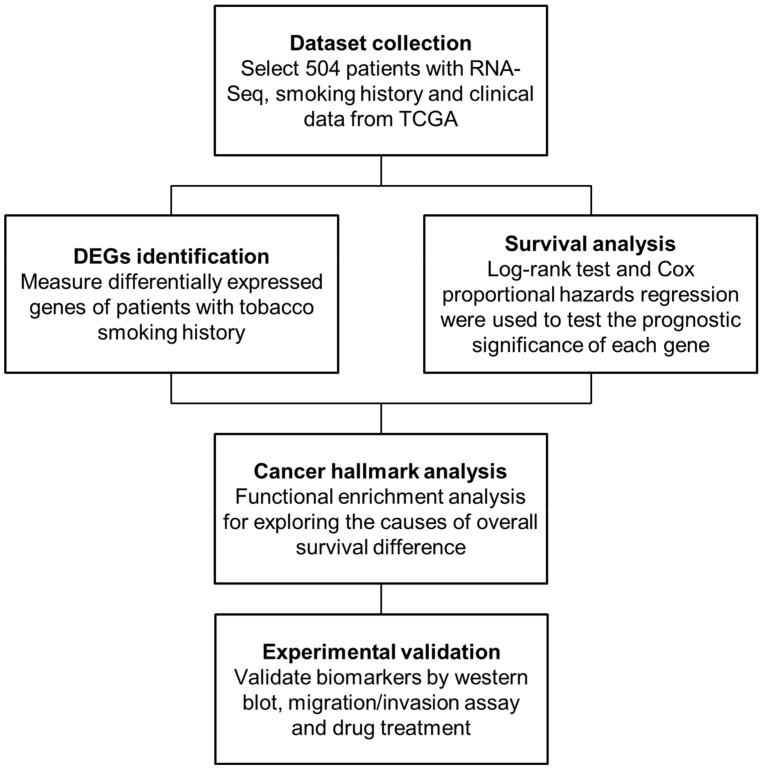
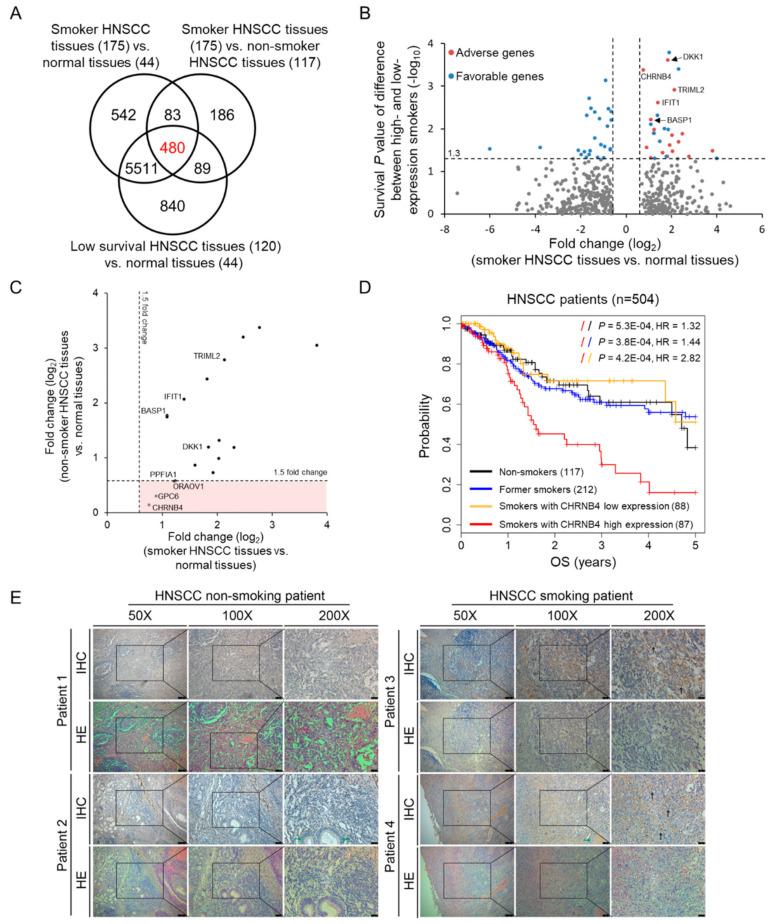
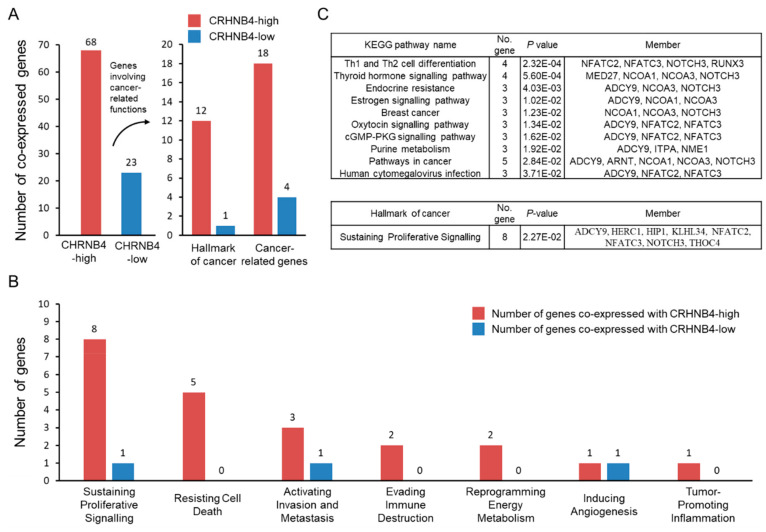
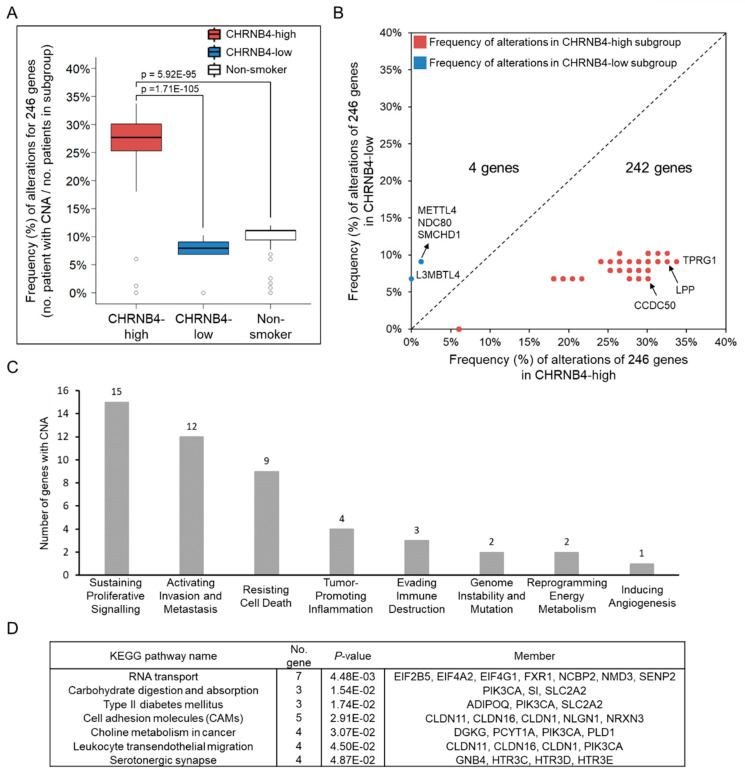
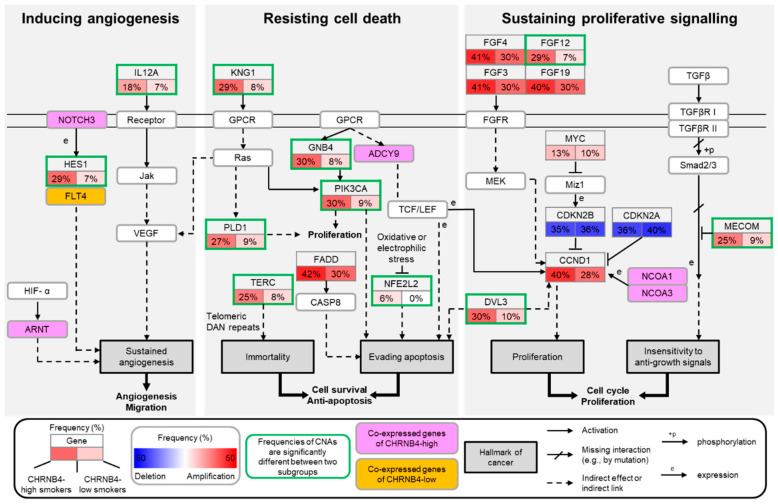
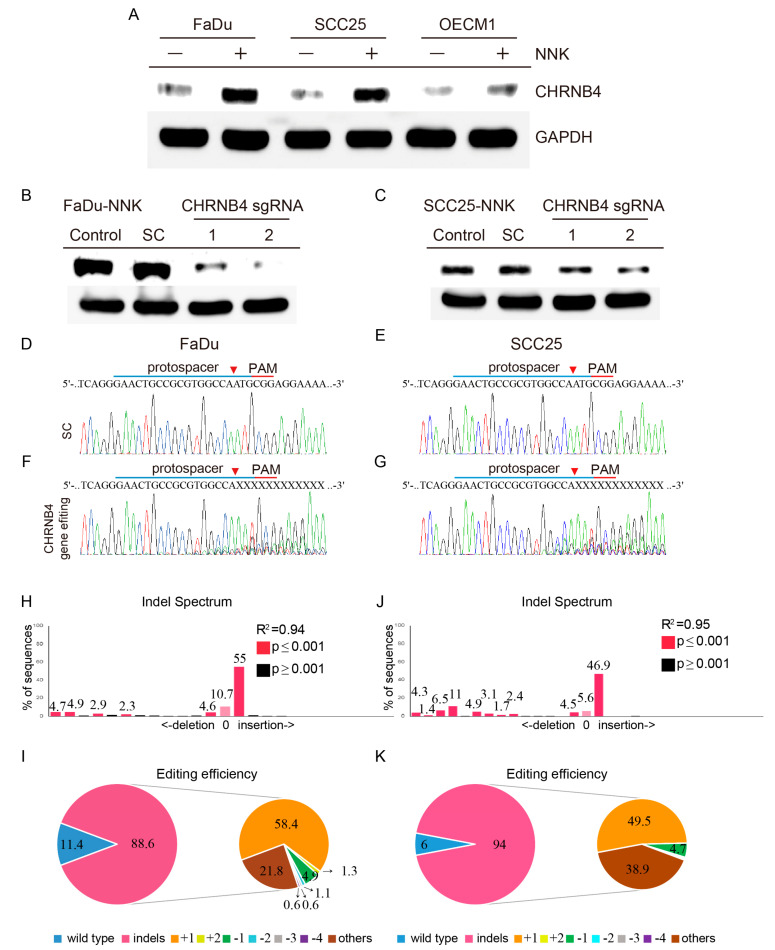
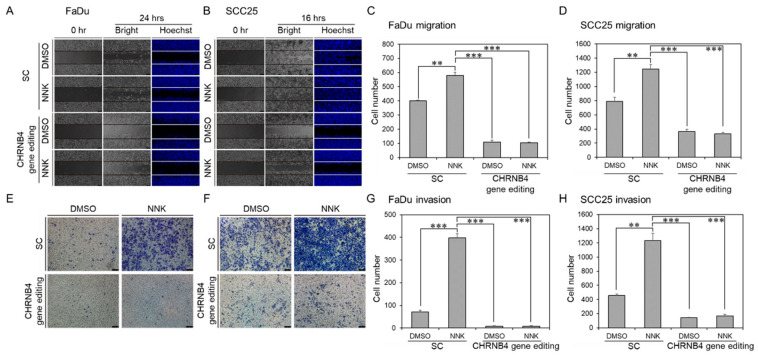
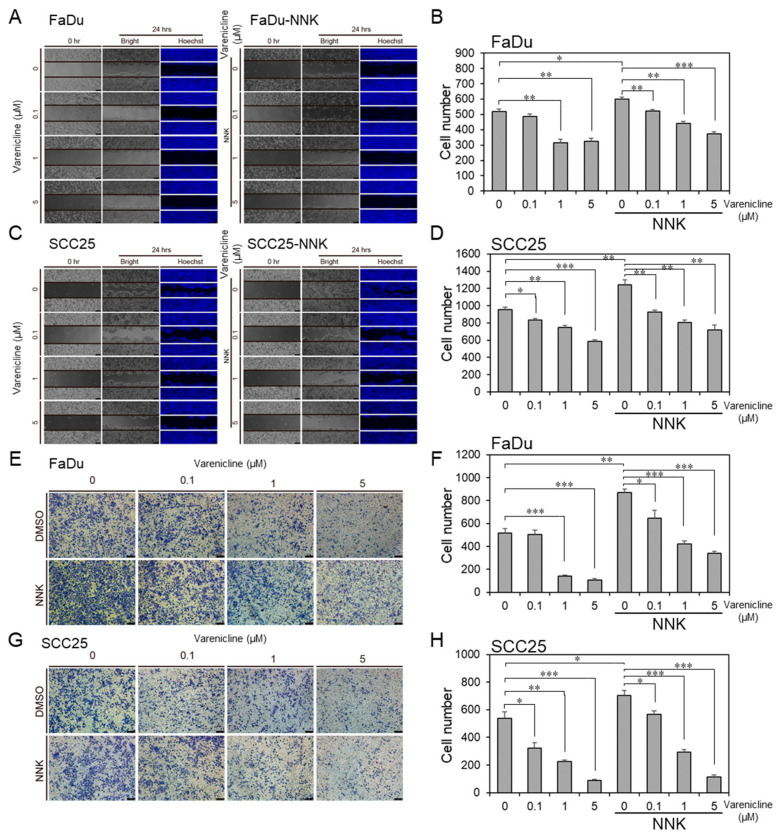
Although many studies have shown the association between smoking and the increased incidence and adverse prognosis of head and neck squamous cell carcinoma (HNSCC), the mechanisms and pharmaceutical targets involved remain unclear. Here, we integrated gene expression signatures, genetic alterations, and survival analyses to identify prognostic indicators and therapeutic targets for smoking HNSCC patients, and we discovered that the FDA-approved drug varenicline inhibits the target for cancer cell migration/invasion. We first identified 18 smoking-related and prognostic genes for HNSCC by using RNA-Seq and clinical follow-up data. One of these genes, CHRNB4 (neuronal acetylcholine receptor subunit beta-4), increased the risk of death by approximately threefold in CHRNB4-high expression smokers compared to CHRNB4-low expression smokers (log rank, p = 0.00042; hazard ratio, 2.82; 95% CI, 1.55-5.14), former smokers, and non-smokers. Furthermore, we examined the functional enrichment of co-regulated genes of CHRNB4 and its 246 frequently occurring copy number alterations (CNAs). We found that these genes were involved in promoting angiogenesis, resisting cell death, and sustaining proliferation, and contributed to much worse outcomes for CHRNB4-high patients. Finally, we performed CHRNB4 gene editing and drug inhibition assays, and the results validate these observations. In summary, our study suggests that CHRNB4 is a prognostic indicator for smoking HNSCC patients and provides a potential new therapeutic drug to prevent recurrence or distant metastasis.
Keywords: drug repurposing; head and neck squamous cell carcinoma (HNSCC); nicotine; prognostic biomarker; smoking.
Conflict of interest statement
The authors have declared no competing interests.
Figures
Similar articles
-
Identification of CHRNB4 as a Diagnostic/Prognostic Indicator and Therapeutic Target in Human Esophageal Squamous Cell Carcinoma.Front Oncol. 2020 Nov 16;10:571167. doi: 10.3389/fonc.2020.571167. eCollection 2020. Front Oncol. 2020. PMID: 33304845 Free PMC article.
-
A prognostic mRNA expression signature of four 16q24.3 genes in radio(chemo)therapy-treated head and neck squamous cell carcinoma (HNSCC).Mol Oncol. 2018 Dec;12(12):2085-2101. doi: 10.1002/1878-0261.12388. Epub 2018 Oct 26. Mol Oncol. 2018. PMID: 30259648 Free PMC article.
-
Gene-expression signature regulated by the KEAP1-NRF2-CUL3 axis is associated with a poor prognosis in head and neck squamous cell cancer.BMC Cancer. 2018 Jan 6;18(1):46. doi: 10.1186/s12885-017-3907-z. BMC Cancer. 2018. PMID: 29306329 Free PMC article.
-
Transcriptomic analysis reveals key lncRNAs associated with ribosomal biogenesis and epidermis differentiation in head and neck squamous cell carcinoma.J Zhejiang Univ Sci B. 2018 Sept.;19(9):674-688. doi: 10.1631/jzus.B1700319. J Zhejiang Univ Sci B. 2018. PMID: 30178634 Free PMC article.
-
The prognostic role of PD-L1 expression for survival in head and neck squamous cell carcinoma: A systematic review and meta-analysis.Oral Oncol. 2018 Nov;86:81-90. doi: 10.1016/j.oraloncology.2018.09.016. Epub 2018 Sep 17. Oral Oncol. 2018. PMID: 30409325
Cited by
-
Gene set correlation enrichment analysis for interpreting and annotating gene expression profiles.Nucleic Acids Res. 2024 Feb 9;52(3):e17. doi: 10.1093/nar/gkad1187. Nucleic Acids Res. 2024. PMID: 38096046 Free PMC article.
-
Transcriptomics and Prognosis Analysis to Identify Critical Biomarkers in Invasive Breast Carcinoma.Technol Cancer Res Treat. 2020 Jan-Dec;19:1533033820957011. doi: 10.1177/1533033820957011. Technol Cancer Res Treat. 2020. PMID: 33176622 Free PMC article.
-
Identification of transcription factors associated with the disease-free survival of triple-negative breast cancer through weighted gene co-expression network analysis.Cytojournal. 2024 Dec 23;21:71. doi: 10.25259/Cytojournal_127_2024. eCollection 2024. Cytojournal. 2024. PMID: 39917004 Free PMC article.
-
Understanding the role of nerves in head and neck cancers - a review.Oncol Rev. 2025 Jan 20;18:1514004. doi: 10.3389/or.2024.1514004. eCollection 2024. Oncol Rev. 2025. PMID: 39906323 Free PMC article. Review.
References
-
- Lohavanichbutr P., Houck J., Fan W., Yueh B., Mendez E., Futran N., Doody D.R., Upton M.P., Farwell D.G., Schwartz S.M., et al. Genomewide Gene Expression Profiles of Hpv-Positive and Hpv-Negative Oropharyngeal Cancer: Potential Implications for Treatment Choices. Arch. Otolaryngol. Head Neck Surg. 2009;135:180–188. doi: 10.1001/archoto.2008.540. - DOI - PMC - PubMed
Grants and funding
- 108-2634-F-009-012/Ministry of Science and Technology, Taiwan
- 107-2314-B-016-028/Ministry of Science and Technology, Taiwan
- 108-2636-B-009-005/Ministry of Science and Technology, Taiwan
- AS-KPQ-105-TPP/Taiwan Protein Project (TPP) of Academia Sinica in Taiwan
- the Center for Intelligent Drug Systems and Smart Bio-devices (IDS2B)/Higher Education Sprout Project by the Ministry of Education (MOE) in Taiwan
LinkOut - more resources
Full Text Sources
Research Materials
