

Hormonal Treatments for Major Depressive Disorder: State of the Art
- PMID: 32456504
- PMCID: PMC7841732
- DOI: 10.1176/appi.ajp.2020.19080848
Hormonal Treatments for Major Depressive Disorder: State of the Art
Erratum in
-
Correction to Dwyer et al.Am J Psychiatry. 2020 Jul 1;177(7):642. doi: 10.1176/appi.ajp.2020.19080848correction. Am J Psychiatry. 2020. PMID: 32605441 No abstract available.
-
Correction to Dwyer et al.Am J Psychiatry. 2020 Oct 1;177(10):1009. doi: 10.1176/appi.ajp.2020.17710correction. Am J Psychiatry. 2020. PMID: 32998544 No abstract available.
Abstract
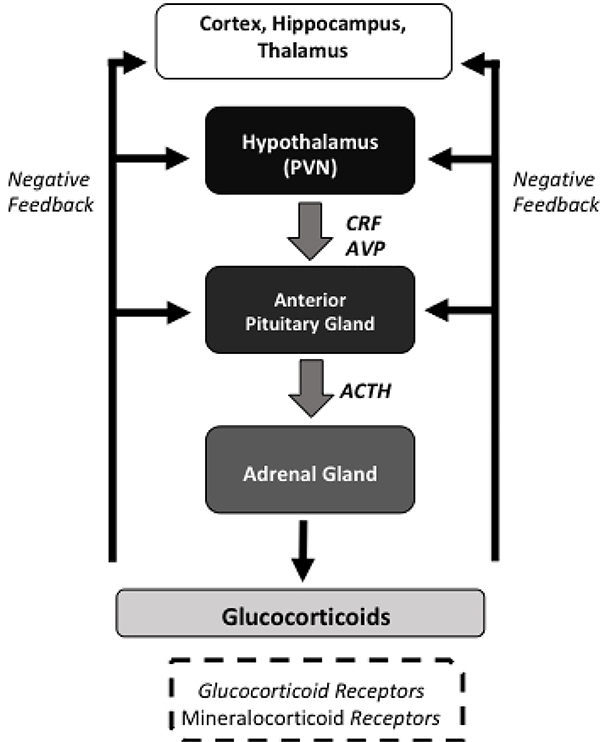
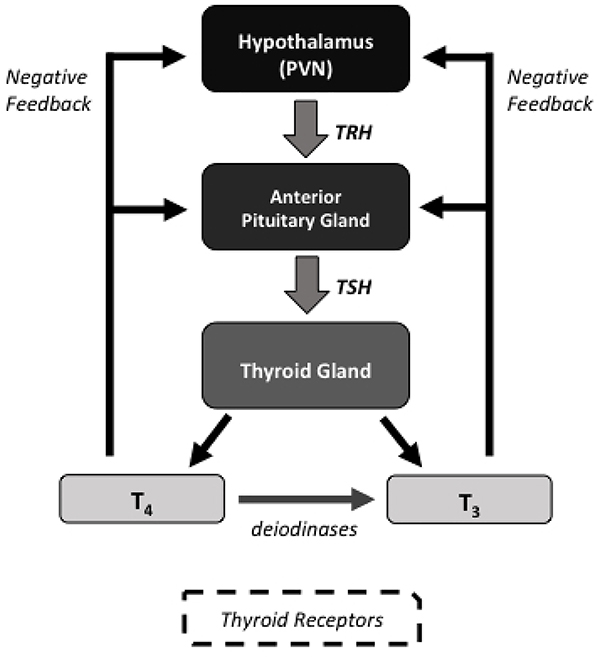
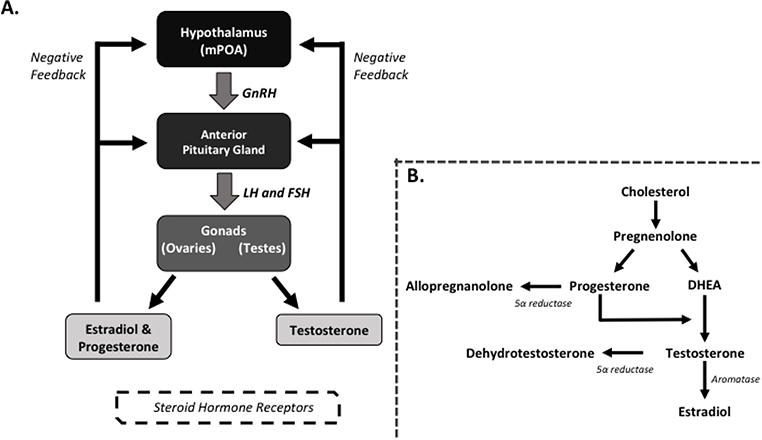
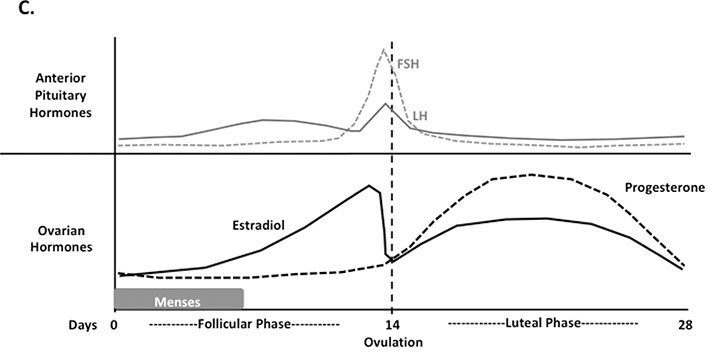
Major depressive disorder is a common psychiatric disorder associated with marked suffering, morbidity, mortality, and cost. The World Health Organization projects that by 2030, major depression will be the leading cause of disease burden worldwide. While numerous treatments for major depression exist, many patients do not respond adequately to traditional antidepressants. Thus, more effective treatments for major depression are needed, and targeting certain hormonal systems is a conceptually based approach that has shown promise in the treatment of this disorder. A number of hormones and hormone-manipulating compounds have been evaluated as monotherapies or adjunctive treatments for major depression, with therapeutic actions attributable not only to the modulation of endocrine systems in the periphery but also to the CNS effects of hormones on non-endocrine brain circuitry. The authors describe the physiology of the hypothalamic-pituitary-adrenal (HPA), hypothalamic-pituitary thyroid (HPT), and hypothalamic-pituitary-gonadal (HPG) axes and review the evidence for selected hormone-based interventions for the treatment of depression in order to provide an update on the state of this field for clinicians and researchers. The review focuses on the HPA axis-based interventions of corticotropin-releasing factor antagonists and the glucocorticoid receptor antagonist mifepristone, the HPT axis-based treatments of thyroid hormones (T3 and T4), and the HPG axis-based treatments of estrogen replacement therapy, the progesterone derivative allopregnanolone, and testosterone. While some treatments have largely failed to translate from preclinical studies, others have shown promising initial results and represent active fields of study in the search for novel effective treatments for major depression.
Keywords: Antidepressants; Neuroendocrinology.
Figures
Comment in
-
Hormone gegen Depression: Stand der Dinge.MMW Fortschr Med. 2020 Nov;162(Suppl 3):26-27. doi: 10.1007/s15006-020-4565-7. MMW Fortschr Med. 2020. PMID: 33164180 Review. German. No abstract available.
References
-
- APA: Diagnostic and statistical manual of mental disorders. 5th ed. Arlington, VA, American Psychiatric Association; 2013.
-
- Greenberg PE, Fournier AA, Sisitsky T, Pike CT, Kessler RC. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). The Journal of clinical psychiatry. 2015;76:155–162. - PubMed
-
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-ofonset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of general psychiatry. 2005;62:593–602. - PubMed
-
- Kessler RC, McGonagle KA, Swartz M, Blazer DG, Nelson CB. Sex and depression in the National Comorbidity Survey. I: Lifetime prevalence, chronicity and recurrence. Journal of affective disorders. 1993;29:85–96. - PubMed
-
- Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, Rush AJ, Walters EE, Wang PS, National Comorbidity Survey R. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). Jama. 2003;289:3095–3105. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
