

Temporal Trends in Percutaneous Coronary Intervention and Coronary Artery Bypass Grafting: Insights From the Washington Cardiac Care Outcomes Assessment Program
- PMID: 32456522
- PMCID: PMC7429009
- DOI: 10.1161/JAHA.119.015317
Temporal Trends in Percutaneous Coronary Intervention and Coronary Artery Bypass Grafting: Insights From the Washington Cardiac Care Outcomes Assessment Program
Abstract
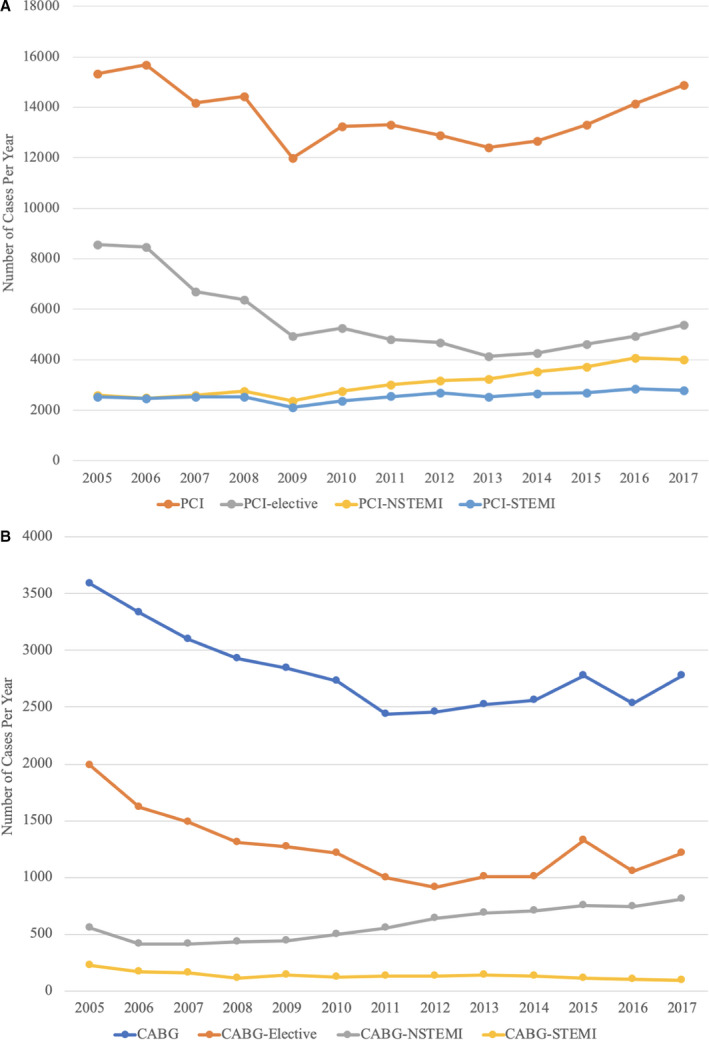
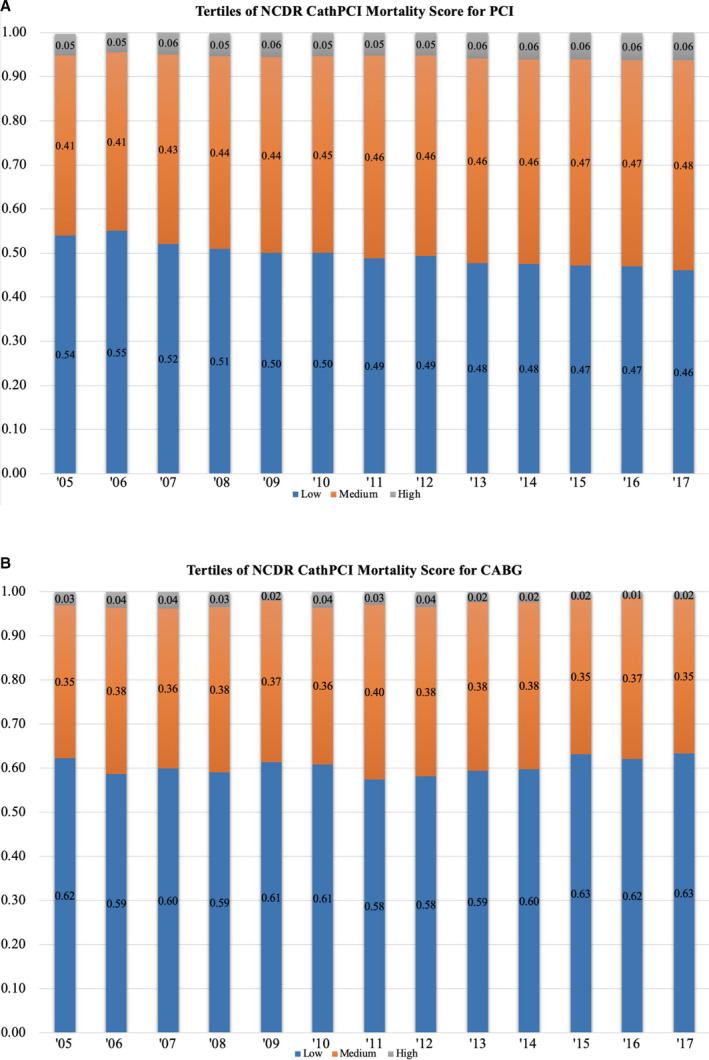
Background Patient selection and outcomes for percutaneous coronary intervention (PCI) and coronary artery bypass grafting (CABG) have changed over the past decade. However, there is limited information on outcomes for both revascularization strategies in the same population. The study evaluated temporal changes in risk profile, procedural characteristics, and clinical outcomes for PCI- and CABG-treated patients. Methods and Results We analyzed all PCI and isolated CABG between 2005 and 2017 in nonfederal hospitals in Washington State. Descriptive analysis was performed to evaluate temporal changes in risk profile and, risk-adjusted in-hospital mortality. Over the study period, 178 474 PCI and 36 592 CABG procedures were performed. PCI and CABG volume decreased by 2.9% and 22.6%, respectively. Compared with 2005-2009, patients receiving either form of revascularization between 2014 and 2017 had a higher prevalence of comorbidities including diabetes mellitus and hypertension and dialysis. Presentation with ST-segment-elevation myocardial infarction (17% versus 20%) and cardiogenic shock (2.4% versus 3.4%) increased for patients with PCI compared with CABG. Conversely, clinical acuity decreased for patients receiving CABG over the study period. From 2005 to 2017, mean National Cardiovascular Data Registry CathPCI mortality score increased for patients treated with PCI (20.1 versus 22.4, P<0.0001) and decreased for patients treated with CABG (18.8 versus 17.8, P<0.0001). Adjusted observed/expected in-hospital mortality ratio increased for PCI (0.98 versus 1.19, P<0.0001) but decreased for CABG (1.21 versus 0.74, P<0.0001) over the study period. Conclusions Clinical acuity increased for patients treated with PCI rather than CABG. This resulted in an increase in adjusted observed/expected mortality ratio for patients undergoing PCI and a decrease for CABG. These shifts may reflect an increased use of PCI instead of CABG for patients considered to be at high surgical risk.
Keywords: bypass surgery; outcomes; percutaneous coronary intervention.
Figures

Comment in
-
Fall and Rise of Coronary Intervention.J Am Heart Assoc. 2020 Jun 2;9(11):e016853. doi: 10.1161/JAHA.120.016853. Epub 2020 May 27. J Am Heart Assoc. 2020. PMID: 32458708 Free PMC article. No abstract available.
References
-
- Boden WE, O'Rourke RA, Teo KK, Hartigan PM, Maron DJ, Kostuk WJ, Knudtson M, Dada M, Casperson P, Harris CL, et al Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356:1503–1516. - PubMed
-
- Yeh RW, Sidney S, Chandra M, Sorel M, Selby JV, Go AS. Population trends in the incidence and outcomes of acute myocardial infarction. N Engl J Med. 2010;362:2155–2165. - PubMed
-
- Cornwell LD, Omer S, Rosengart T, Holman WL, Bakaeen FG. Changes over time in risk profiles of patients who undergo coronary artery bypass graft surgery: the veterans affairs surgical quality improvement program (VASQIP). JAMA Surg. 2015;150:308–315. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
