

Serum free thiols predict cardiovascular events and all-cause mortality in the general population: a prospective cohort study
- PMID: 32456645
- PMCID: PMC7251849
- DOI: 10.1186/s12916-020-01587-w
Serum free thiols predict cardiovascular events and all-cause mortality in the general population: a prospective cohort study
Abstract
Background: Serum free thiols (R-SH, sulfhydryl groups) reliably reflect systemic oxidative stress. Since serum free thiols are rapidly oxidized by reactive species, systemic oxidative stress is generally associated with reduced serum free thiol levels. Free thiols associate with favorable disease outcomes in many patient cohorts, and the current hypothesis is that oxidative stress might also play an important role in cardiovascular disease. In this study, we aimed to establish the role of serum free thiols in the general population by investigating their relationship with the risk of cardiovascular (CV) events and all-cause mortality.
Methods: Participants (n = 5955) of the Prevention of REnal and Vascular ENd-stage Disease (PREVEND) cohort study from the general population were included. At baseline, serum levels of free thiols were quantified and adjusted to total protein levels. Protein-adjusted serum free thiol levels were studied for their associations with clinical and biochemical parameters, as well as with the risk of CV events and all-cause mortality.
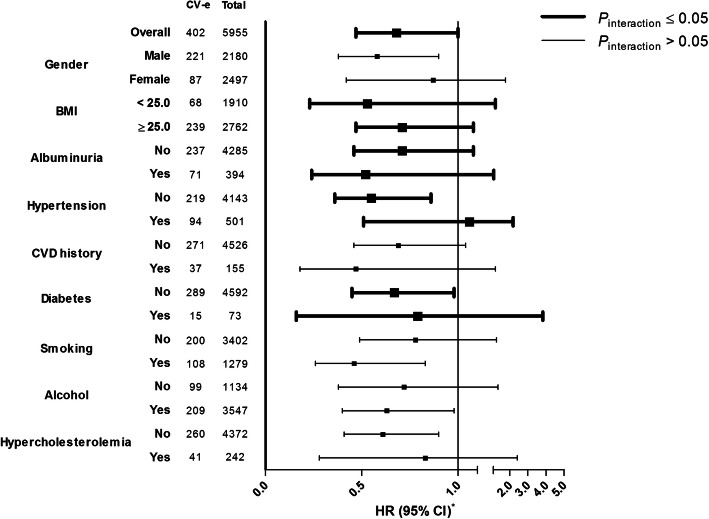
Results: The mean protein-adjusted serum free thiol level was 5.05 ± 1.02 μmol/g of protein. Protein-adjusted serum free thiols significantly predicted the risk of CV events, even after adjustment for potential confounding factors (hazard ratio [HR] per doubling 0.68 [95% confidence interval [CI] 0.47-1.00], P = 0.048). Similarly, protein-adjusted serum free thiols were significantly predictive of the risk of all-cause mortality (HR per doubling 0.66 [95% CI 0.44-1.00], P = 0.050). Stratified analyses revealed lower HRs for subjects with a lower body mass index (BMI), without hypertension, and without diabetes. Conversely, HRs were lower in subjects with albuminuria.
Conclusions: In this large population-based cohort study, serum free thiols significantly predicted the risk of CV events and all-cause mortality. Our results highlight the potential significance and clinical applicability of serum free thiols since they are amendable to therapeutic intervention.
Keywords: Cardiovascular disease; Free thiols; Mortality; Oxidative stress; Population study.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–2128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
-
- Wang H, Naghavi M, Allen C, Barber RM, Carter A, Casey DC, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388:1459–1544. doi: 10.1016/S0140-6736(16)31012-1. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
