

Benzodiazepines, Codispensed Opioids, and Mortality among Patients Initiating Long-Term In-Center Hemodialysis
- PMID: 32457228
- PMCID: PMC7274292
- DOI: 10.2215/CJN.13341019
Benzodiazepines, Codispensed Opioids, and Mortality among Patients Initiating Long-Term In-Center Hemodialysis
Abstract
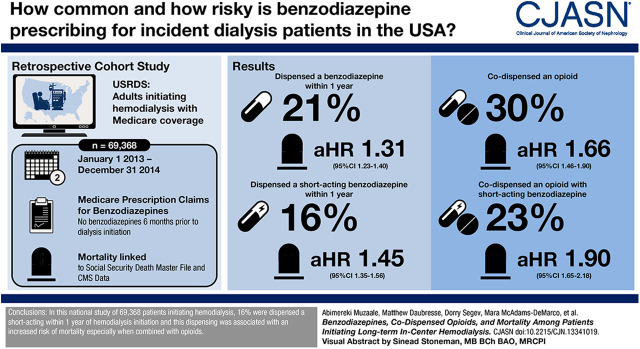
Background and objectives: Mortality from benzodiazepine/opioid interactions is a growing concern in light of the opioid epidemic. Patients on hemodialysis suffer from a high burden of physical/psychiatric conditions, which are treated with benzodiazepines, and they are three times more likely to be prescribed opioids than the general population. Therefore, we studied mortality risk associated with short- and long-acting benzodiazepines and their interaction with opioids among adults initiating hemodialysis.
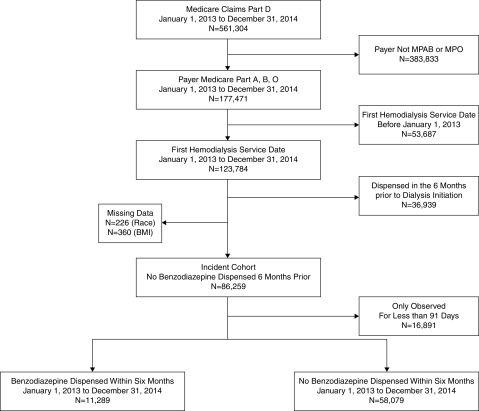
Design, setting, participants, & measurements: The cohort of 69,368 adults initiating hemodialysis (January 2013 to December 2014) was assembled by linking US Renal Data System records to Medicare claims. Medicare claims were used to identify dispensed benzodiazepines and opioids. Using adjusted Cox proportional hazards models, we estimated the mortality risk associated with benzodiazepines (time varying) and tested whether the benzodiazepine-related mortality risk differed by opioid codispensing.
Results: Within 1 year of hemodialysis initiation, 10,854 (16%) patients were dispensed a short-acting benzodiazepine, and 3262 (5%) patients were dispensed a long-acting benzodiazepine. Among those who were dispensed a benzodiazepine during follow-up, codispensing of opioids and short-acting benzodiazepines occurred among 3819 (26%) patients, and codispensing of opioids and long-acting benzodiazepines occurred among 1238 (8%) patients. Patients with an opioid prescription were more likely to be subsequently dispensed a short-acting benzodiazepine (adjusted hazard ratio, 1.66; 95% confidence interval, 1.59 to 1.74) or a long-acting benzodiazepine (adjusted hazard ratio, 1.11; 95% confidence interval, 1.03 to 1.20). Patients dispensed a short-acting benzodiazepine were at a 1.45-fold (95% confidence interval, 1.35 to 1.56) higher mortality risk compared with those without a short-acting benzodiazepine; among those with opioid codispensing, this risk was 1.90-fold (95% confidence interval, 1.65 to 2.18; Pinteraction<0.001). In contrast, long-acting benzodiazepine dispensing was inversely associated with mortality (adjusted hazard ratio, 0.84; 95% confidence interval, 0.72 to 0.99) compared with no dispensing of long-acting benzodiazepine; there was no differential risk by opioid dispensing (Pinteraction=0.72).
Conclusions: Codispensing of opioids and short-acting benzodiazepines is common among patients on dialysis, and it is associated with higher risk of death.
Keywords: Analgesics; Benzodiazepines; Cohort Studies; Follow-Up Studies; Medicare; Opioid; Opioid Epidemic; Prescriptions; Proportional Hazards Models; Records; dialysis; renal dialysis.
Copyright © 2020 by the American Society of Nephrology.
Figures
Comment in
-
A Patient's Perspective on Benzodiazepines, Co-Dispensed Opioids, and Mortality among Patients Initiating Long-Term In-Center Hemodialysis.Clin J Am Soc Nephrol. 2020 Jun 8;15(6):743-744. doi: 10.2215/CJN.05150420. Epub 2020 May 26. Clin J Am Soc Nephrol. 2020. PMID: 32458812 Free PMC article. No abstract available.
References
-
- Cunningham CM, Hanley GE, Morgan S: Patterns in the use of benzodiazepines in British Columbia: Examining the impact of increasing research and guideline cautions against long-term use. Health Policy 97: 122–129, 2010 - PubMed
-
- Olfson M, King M, Schoenbaum M: Benzodiazepine use in the United States. JAMA Psychiatry 72: 136–142, 2015 - PubMed
-
- Jones CM, McAninch JK: Emergency department visits and overdose deaths from combined use of opioids and benzodiazepines. Am J Prev Med 49: 493–501, 2015 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
