

Fasting-Induced Natriuresis and SGLT: A New Hypothesis for an Old Enigma
- PMID: 32457696
- PMCID: PMC7221140
- DOI: 10.3389/fendo.2020.00217
Fasting-Induced Natriuresis and SGLT: A New Hypothesis for an Old Enigma
Abstract
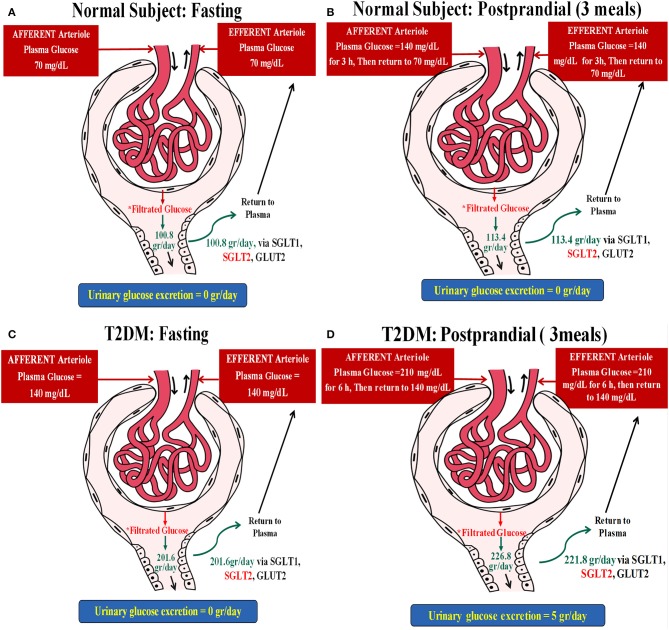
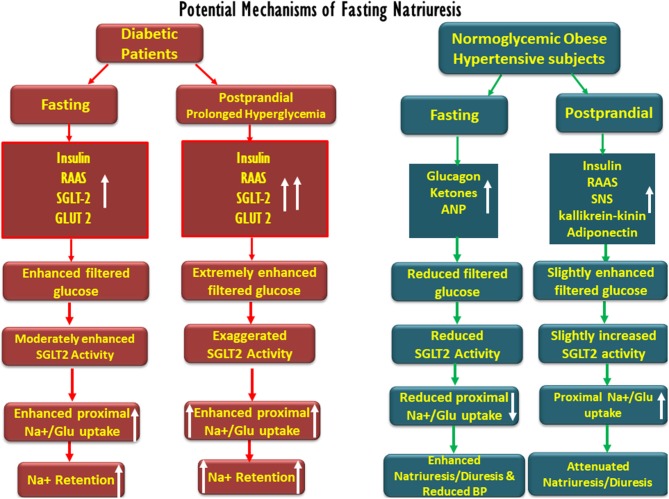
For years, physicians and scientists were enthralled by the enigmatic phenomenon of fasting-associated diuresis and natriuresis and their reversal by feeding. This abrupt response is most prominent in obese and hypertensive individuals, and if repeated once and again may lead to the attenuation of blood pressure and improve insulin sensitivity. The mechanisms involved in early natriuresis and diuresis remain speculative as the renin-angiotensin-aldosterone axis and natriuretic peptides are initially suppressed. Based on gained insight using sodium-glucose transporter 2 (SGLT-2) inhibitors, herein, we propose a role for enhanced post-prandial proximal tubular sodium uptake, mediated by increased glucose-sodium co-transport, as daily filtered glucose increases, and reduced sodium uptake when glucose reabsorption diminishes. This phenomenon might be more pronounced in diabetics due to prolonged post-prandial hyperglycemia and intense SGLT-driven transport. Our hypothesis may also provide a physiologic basis for fasting-related reduced blood pressure in hypertension. This theory deserves challenging by experimental and clinical studies.
Keywords: SGLT-2; diabetes; fasting; glucose; hypertension; natriuresis; obesity; sodium.
Copyright © 2020 Heyman, Bursztyn, Szalat, Muszkat and Abassi.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous