

Therapeutic Potential of Combining PARP Inhibitor and Immunotherapy in Solid Tumors
- PMID: 32457830
- PMCID: PMC7228136
- DOI: 10.3389/fonc.2020.00570
Therapeutic Potential of Combining PARP Inhibitor and Immunotherapy in Solid Tumors
Abstract
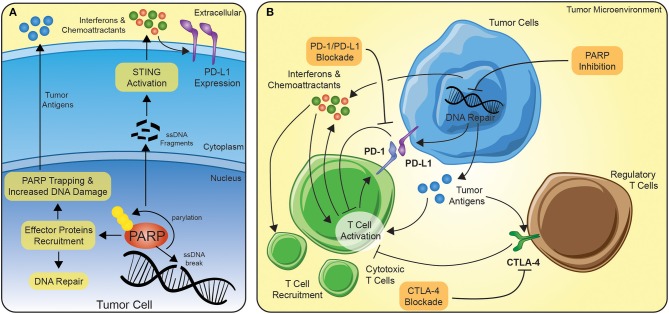
Immunotherapy has revolutionized the treatment of both hematological malignancies and solid tumors. The use of immunotherapy has improved outcome for patients with cancer across multiple tumor types, including lung, melanoma, ovarian, genitourinary, and more recently breast cancer with durable responses seen even in patients with widespread metastatic disease. Despite the promising results, immunotherapy still helps only a subset of patients due to overall low response rates. Moreover, the response to immunotherapy is highly cancer specific and results have not been as promising in cancers that are considered less immunogenic. The strategies to improve immunotherapy responses have focused on biomarker selection, like PD-L1 status, and usage of combinatorial agents, such as chemotherapy, targeted therapy, and radiotherapy. Of particular interest, DNA-damaging agents have the potential to enhance the response to immunotherapy by promoting neoantigen release, increasing tumor mutational burden, and enhancing PD-L1 expression. Poly-ADP-ribose polymerase (PARP) inhibitors are one such class of drugs that has shown synergy with immunotherapy in preclinical and early clinical studies. PARP-based therapies work through the inhibition of single-strand DNA repair leading to DNA damage, increased tumor mutational burden, making the tumor a more attractive target for immunotherapy. Of the solid tumors reviewed, breast, ovarian, and prostate cancers have demonstrated efficacy in the combination of PARP inhibition and immunotherapy, predominately in BRCA-mutated tumors. However, initial investigations into wildtype BRCA and gastrointestinal tumors have shown moderate overall response or disease control rates, dependent on the tumor type. In contrast, although a number of clinical trials underway, there is a paucity of published results for the use of the combination in lung or urothelial cancers. Overall this article focuses on the promise of combinatorial PARP inhibition and immunotherapy to improve patient outcomes in solid tumors, summarizing both early results and looking toward ongoing trials.
Keywords: PARP inhibitor; breast cancer; combination therapy; gastrointestinal cancers; gynecologic cancer; immunotherapy; prostate cancer; solid tumors.
Copyright © 2020 Vikas, Borcherding, Chennamadhavuni and Garje.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials