

First episode psychosis: register-based study of comorbid psychiatric disorders and medications before and after
- PMID: 32458108
- PMCID: PMC7960599
- DOI: 10.1007/s00406-020-01139-6
First episode psychosis: register-based study of comorbid psychiatric disorders and medications before and after
Abstract
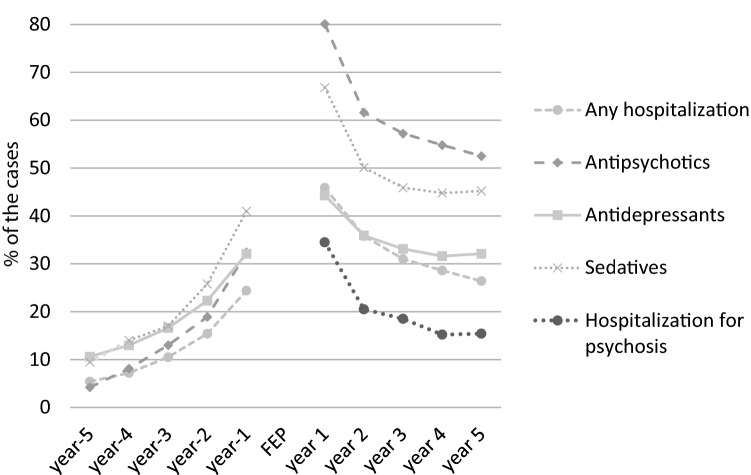
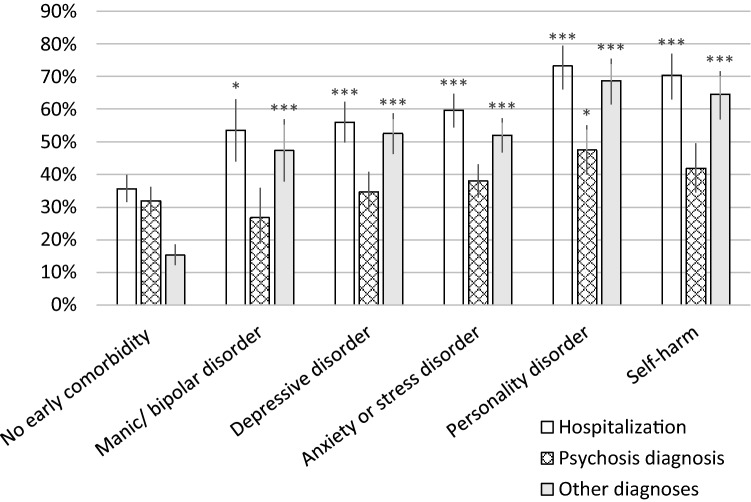
Comorbid psychiatric disorders are common in first episode psychosis. We investigated comorbid disorders before, at, and after a first hospital-treated psychosis in a naturalistic nation-wide cohort (n = 2091) with a first psychosis hospitalization between 2007 and 2011, and at ages between 16 and 25. Swedish population registers were used to identify the cohort and to collect data on diagnoses at hospitalizations and medications. The proportions of cases with hospitalizations or medications increased year by year before and decreased in the years after the first psychosis hospitalization. In the 2 years before, 30% had hospitalizations with other psychiatric diagnoses and 60% had psychiatric medications. At the first psychosis hospitalization, 46% had other comorbid psychiatric diagnoses or self-harm. In the 2 years before or at the first psychosis hospitalization, 17% had anxiety or stress disorders at hospitalizations, 12% depressive disorders, 5.4% manic or bipolar disorders, 8.6% personality disorders, 26% substance use disorders, and 15% neurodevelopmental disorders. 8.2% had hospitalizations for self-harm. At most, around 30% of the cases were estimated not to have had any comorbid psychiatric disorders before or at the first psychosis presentation. Early comorbid affective, anxiety or personality disorders or self-harm were associated with a worse outcome, as measured by new psychiatric hospitalizations. The outcome was worst for personality disorders with 73% re-hospitalizations within 1 year and for patients with self-harm with 70% re-hospitalizations. In conclusion, most cases with a first psychosis hospitalization had clinical presentations indicating comorbid psychiatric disorders. Cases with comorbidity had a higher risk for re-hospitalizations.
Keywords: Affective disorder; Anxiety; Personality disorder; Schizophrenia; Self-harm.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
