

Management of acute pulmonary embolism 2019: what is new in the updated European guidelines?
- PMID: 32458205
- PMCID: PMC7467952
- DOI: 10.1007/s11739-020-02340-0
Management of acute pulmonary embolism 2019: what is new in the updated European guidelines?
Abstract
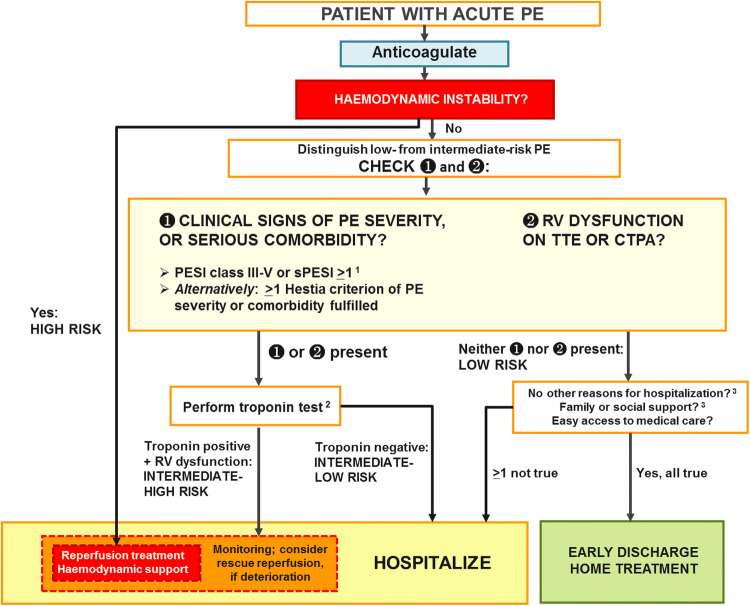
Pulmonary embolism (PE) is the third most frequent acute cardiovascular syndrome. Annual PE incidence and PE-related mortality rates rise exponentially with age, and consequently, the disease burden imposed by PE on the society continues to rise as the population ages worldwide. Recently published landmark trials provided the basis for new or changed recommendations included in the 2019 update of the European Society of Cardiology Guidelines (developed in cooperation with the European Respiratory Society). Refinements in diagnostic algorithms were proposed and validated, increasing the specificity of pre-test clinical probability and D-dimer testing, and thus helping to avoid unnecessary pulmonary angiograms. Improved diagnostic strategies were also successfully tested in pregnant women with suspected PE. Non-vitamin K antagonist oral anticoagulants (NOACs) are now the preferred agents for treating the majority of patients with PE, both in the acute phase (with or without a brief lead-in period of parenteral heparin or fondaparinux) and over the long term. Primary reperfusion is reserved for haemodynamically unstable patients. Besides, the 2019 Guidelines endorse multidisciplinary teams for coordinating the acute-phase management of high-risk and (in selected cases) intermediate-risk PE. For normotensive patients, physicians are advised to include the assessment of the right ventricle on top of clinical severity scores in further risk stratification, especially if early discharge of the patient is envisaged. Further important updates include guidance (1) on extended anticoagulation after PE, taking into account the improved safety profile of NOACs; and (2) on the overall care and follow-up of patients who have suffered PE, with the aim to prevent, detect and treat late sequelae of venous thromboembolism.
Keywords: Anticoagulation; Diagnosis; Guidelines; Pulmonary embolism; Treatment.
Conflict of interest statement
Dr. Konstantinides reports research grants from Bayer AG, Boehringer Ingelheim, Actelion Janssen, Daiichi Sankyo; educational grants from Biocompatibles Group UK - Boston Scientific, Daiichi Sankyo; lecture and consultation fees from Bayer AG, Pfizer-Bristol-Myers Squibb, MSD, Servier - all outside the submitted work.
Figures
References
-
- Raskob GE, Angchaisuksiri P, Blanco AN, Buller H, Gallus A, Hunt BJ, et al. Thrombosis: a major contributor to global disease burden. Arterioscler Thromb Vasc Biol. 2014;34(11):2363–2371. - PubMed
-
- Wendelboe AM, Raskob GE. Global burden of thrombosis: epidemiologic aspects. Circ Res. 2016;118(9):1340–1347. - PubMed
-
- de Miguel-Diez J, Jimenez-Garcia R, Jimenez D, Monreal M, Guijarro R, Otero R, et al. Trends in hospital admissions for pulmonary embolism in Spain from 2002 to 2011. Eur Respir J. 2014;44(4):942–950. - PubMed
-
- Dentali F, Ageno W, Pomero F, Fenoglio L, Squizzato A, Bonzini M. Time trends and case fatality rate of in-hospital treated pulmonary embolism during 11 years of observation in Northwestern Italy. Thromb Haemost. 2016;115(2):399–405. - PubMed
-
- Lehnert P, Lange T, Moller CH, Olsen PS, Carlsen J. Acute pulmonary embolism in a national Danish cohort: increasing incidence and decreasing mortality. Thromb Haemost. 2018;118(3):539–546. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
