

Impact of Transport Time and Cardiac Arrest Centers on the Neurological Outcome After Out-of-Hospital Cardiac Arrest: A Retrospective Cohort Study
- PMID: 32458720
- PMCID: PMC7429006
- DOI: 10.1161/JAHA.119.015544
Impact of Transport Time and Cardiac Arrest Centers on the Neurological Outcome After Out-of-Hospital Cardiac Arrest: A Retrospective Cohort Study
Abstract
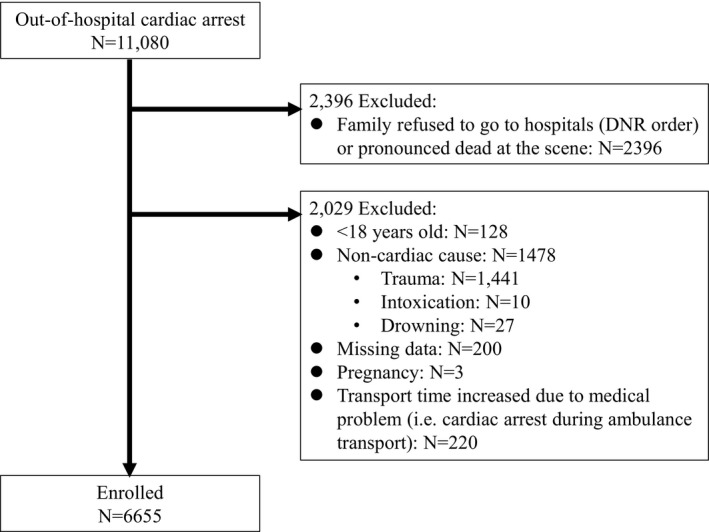
Background Should all out-of-hospital cardiac arrest (OHCA) patients be directly transported to cardiac arrest centers (CACs) remains under debate. Our study evaluated the impacts of different transport time and destination hospital on the outcomes of OHCA patients. Methods and Results Data were collected from 6655 OHCA patients recorded in the regional prospective OHCA registry database of Taoyuan City, Taiwan, between January 2012 and December 2016. Patients were matched on propensity score, which left 5156 patients, 2578 each in the CAC and non-CAC groups. Transport time was dichotomized into <8 and ≥8 minutes. The relations between the transport time to CACs and good neurological outcome at discharge and survival to discharge were investigated. Of the 5156 patients, 4215 (81.7%) presented with nonshockable rhythms and 941 (18.3%) presented with shockable rhythms. Regardless of transport time, transportation to a CAC increased the likelihoods of survival to discharge (<8 minutes: adjusted odds ratio [aOR], 1.95; 95% CI, 1.11-3.41; ≥8 minutes: aOR, 1.92; 95% CI, 1.25-2.94) and good neurological outcome at discharge (<8 minutes: aOR, 2.70; 95% CI, 1.40-5.22; ≥8 minutes: aOR, 2.20; 95% CI, 1.29-3.75) in OHCA patients with shockable rhythms but not in patients with nonshockable rhythms. Conclusions OHCA patients with shockable rhythms transported to CACs demonstrated higher probabilities of survival to discharge and a good neurological outcome at discharge. Direct ambulance delivery to CACs should thus be considered, particularly when OHCA patients present with shockable rhythms.
Keywords: cardiac arrest center; initial rhythm; neurological outcome; out‐of‐hospital cardiac arrest; transport time.
Figures
References
-
- Berdowski J, Berg RA, Tijssen JGP, Koster RW. Global incidences of out‐of‐hospital cardiac arrest and survival rates: systematic review of 67 prospective studies. Resuscitation. 2010;81:1479–1487. - PubMed
-
- Meaney PA, Nadkarni VM, Kern KB, Indik JH, Halperin HR, Berg RA. Rhythms and outcomes of adult in‐hospital cardiac arrest. Crit Care Med. 2010;38:101–108. - PubMed
-
- Nolan J. European resuscitation council guidelines for resuscitation 2005: section 1: introduction. Resuscitation. 2005;67:S3–S6. - PubMed
-
- Sunde K, Pytte M, Jacobsen D, Mangschau A, Jensen LP, Smedsrud C, Draegni T, Steen PA. Implementation of a standardised treatment protocol for post resuscitation care after out‐of‐hospital cardiac arrest. Resuscitation. 2007;73:29–39. - PubMed
-
- Lund‐Kordahl I, Olasveengen TM, Lorem T, Samdal M, Wik L, Sunde K. Improving outcome after out‐of‐hospital cardiac arrest by strengthening weak links of the local Chain of Survival; quality of advanced life support and post‐resuscitation care. Resuscitation. 2010;81:422–426. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
