

Effectiveness of Mobile App-Assisted Self-Care Interventions for Improving Patient Outcomes in Type 2 Diabetes and/or Hypertension: Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 32459654
- PMCID: PMC7435643
- DOI: 10.2196/15779
Effectiveness of Mobile App-Assisted Self-Care Interventions for Improving Patient Outcomes in Type 2 Diabetes and/or Hypertension: Systematic Review and Meta-Analysis of Randomized Controlled Trials
Erratum in
-
Correction: Effectiveness of Mobile App-Assisted Self-Care Interventions for Improving Patient Outcomes in Type 2 Diabetes and/or Hypertension: Systematic Review and Meta-Analysis of Randomized Controlled Trials.JMIR Mhealth Uhealth. 2020 Aug 19;8(8):e23600. doi: 10.2196/23600. JMIR Mhealth Uhealth. 2020. PMID: 32813666 Free PMC article.
Abstract
Background: Mobile app-assisted self-care interventions are emerging promising tools to support self-care of patients with chronic diseases such as type 2 diabetes and hypertension. The effectiveness of such interventions requires further exploration for more supporting evidence.
Objective: A systematic review and meta-analysis of randomized controlled trials (RCTs) were conducted to examine the effectiveness of mobile app-assisted self-care interventions developed for type 2 diabetes and/or hypertension in improving patient outcomes.
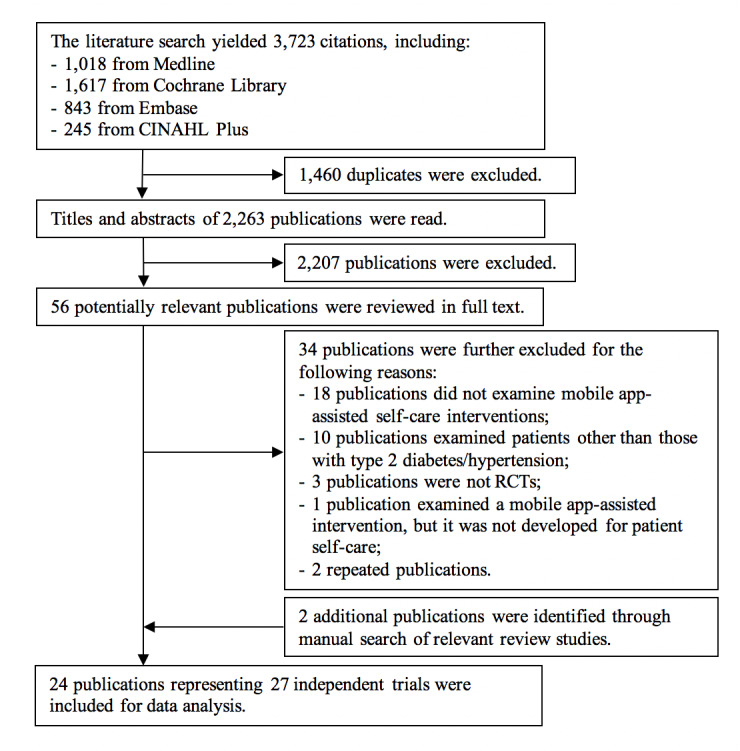
Methods: We followed the Cochrane Collaboration guidelines and searched MEDLINE, Cochrane Library, EMBASE, and CINAHL Plus for relevant studies published between January 2007 and January 2019. Primary outcomes included changes in hemoglobin A1c (HbA1c) levels, systolic blood pressure (SBP), and diastolic blood pressure (DBP). Changes in other clinical-, behavioral-, knowledge-, and psychosocial-related outcomes were included as secondary outcomes. Primary outcomes and objective secondary outcomes that were reported in at least two trials were meta-analyzed; otherwise, a narrative synthesis was used for data analysis.
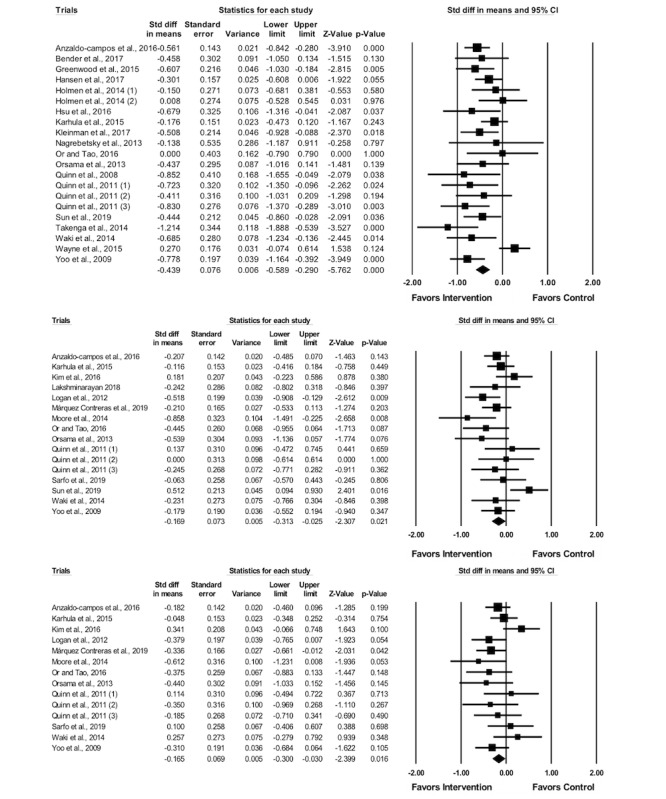
Results: A total of 27 trials were identified and analyzed. For primary outcomes, the use of mobile app-assisted self-care interventions was associated with significant reductions in HbA1c levels (standardized mean difference [SMD] -0.44, 95% CI -0.59 to -0.29; P<.001), SBP (SMD -0.17, 95% CI -0.31 to -0.03, P=.02), and DBP (SMD -0.17, 95% CI -0.30 to -0.03, P=.02). Subgroup analyses for primary outcomes showed that several intervention features were supportive of self-management, including blood glucose, blood pressure, and medication monitoring, communication with health care providers, automated feedback, personalized goal setting, reminders, education materials, and data visualization. In addition, 8 objective secondary outcomes were meta-analyzed, which showed that the interventions had significant lowering effects on fasting blood glucose levels and waist circumference. A total of 42 secondary outcomes were narratively synthesized, and mixed results were found.
Conclusions: Mobile app-assisted self-care interventions can be effective tools for managing blood glucose and blood pressure, likely because their use facilitates remote management of health issues and data, provision of personalized self-care recommendations, patient-care provider communication, and decision making. More studies are required to further determine which combinations of intervention features are most effective in improving the control of the diseases. Moreover, evidence regarding the effects of these interventions on the behavioral, knowledge, and psychosocial outcomes of patients is still scarce, which warrants further examination.
Keywords: hypertension; mobile app; self-care; type 2 diabetes.
©Kaifeng Liu, Zhenzhen Xie, Calvin Kalun Or. Originally published in JMIR mHealth and uHealth (http://mhealth.jmir.org), 04.08.2020.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Diabetes and high blood pressure. Blood Pressure UK. 2008. [2020-02-26]. http://www.bloodpressureuk.org/BloodPressureandyou/Yourbody/Diabetes .
-
- Cheung BMY, Wat NMS, Tso AWK, Tam S, Thomas GN, Leung GM, Tse HF, Woo J, Janus ED, Lau CP, Lam TH, Lam KSL. Association between raised blood pressure and dysglycemia in Hong Kong Chinese. Diabetes Care. 2008 Sep;31(9):1889–1891. doi: 10.2337/dc08-0405. http://europepmc.org/abstract/MED/18556342 dc08-0405 - DOI - PMC - PubMed
-
- Bayliss EA, Steiner JF, Fernald DH, Crane LA, Main DS. Descriptions of barriers to self-care by persons with comorbid chronic diseases. Ann Fam Med. 2003;1(1):15–21. http://www.annfammed.org/cgi/pmidlookup?view=long&pmid=15043175 - PMC - PubMed
-
- El-Gayar O, Timsina P, Nawar N, Eid W. Mobile applications for diabetes self-management: status and potential. J Diabetes Sci Technol. 2013;7(1):247–262. http://europepmc.org/abstract/MED/23439183 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
