

The compensatory phenomenon of the functional connectome related to pathological biomarkers in individuals with subjective cognitive decline
- PMID: 32460888
- PMCID: PMC7254770
- DOI: 10.1186/s40035-020-00201-6
The compensatory phenomenon of the functional connectome related to pathological biomarkers in individuals with subjective cognitive decline
Abstract
Background: Subjective cognitive decline (SCD) is a preclinical stage along the Alzheimer's disease (AD) continuum. However, little is known about the aberrant patterns of connectivity and topological alterations of the brain functional connectome and their diagnostic value in SCD.
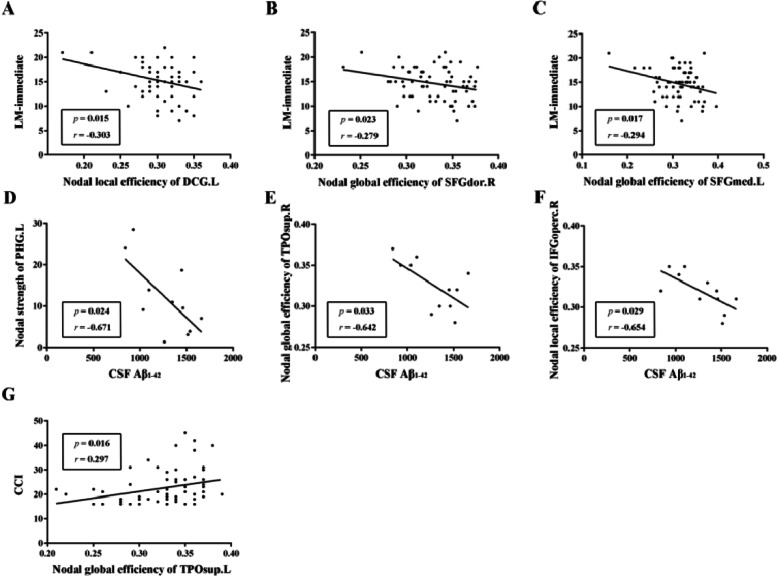
Methods: Resting-state functional magnetic resonance imaging and graph theory analyses were used to investigate the alterations of the functional connectome in 66 SCD individuals and 64 healthy controls (HC). Pearson correlation analysis was computed to assess the relationships among network metrics, neuropsychological performance and pathological biomarkers. Finally, we used the multiple kernel learning-support vector machine (MKL-SVM) to differentiate the SCD and HC individuals.
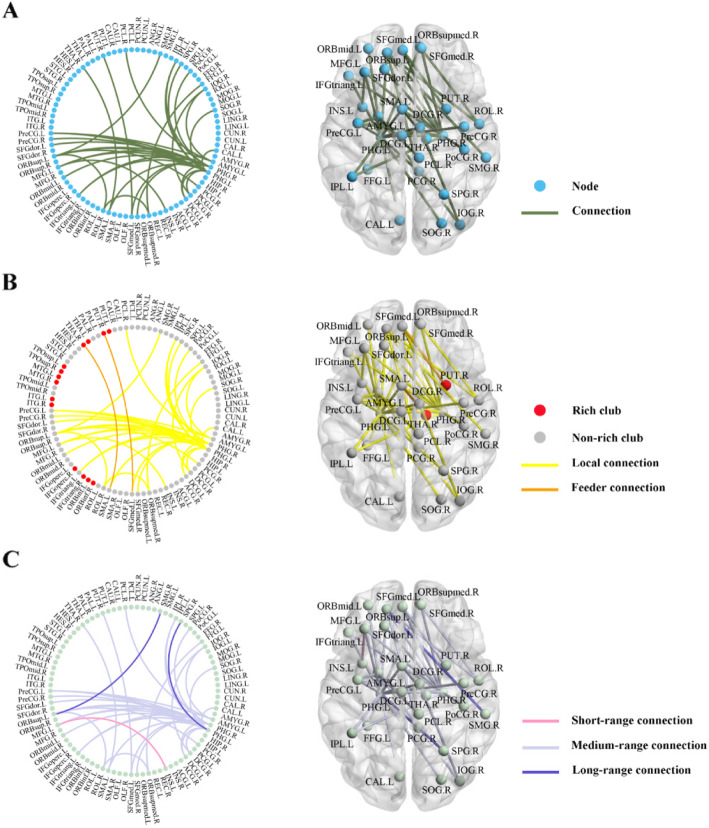
Results: SCD individuals showed higher nodal topological properties (including nodal strength, nodal global efficiency and nodal local efficiency) associated with amyloid-β levels and memory function than the HC, and these regions were mainly located in the default mode network (DMN). Moreover, increased local and medium-range connectivity mainly between the bilateral parahippocampal gyrus (PHG) and other DMN-related regions was found in SCD individuals compared with HC individuals. These aberrant functional network measures exhibited good classification performance in the differentiation of SCD individuals from HC individuals at an accuracy up to 79.23%.
Conclusion: The findings of this study provide insight into the compensatory mechanism of the functional connectome underlying SCD. The proposed classification method highlights the potential of connectome-based metrics for the identification of the preclinical stage of AD.
Keywords: Compensatory mechanism; Machine learning; Subjective cognitive decline; rs-fMRI.
Conflict of interest statement
The authors have declared that no competing interest exists.
Figures



References
-
- Scheltens P, Blennow K, Breteler MM, de Strooper B, Frisoni GB, Salloway S, Van der Flier WM. Alzheimer’s disease. Lancet. 2016;388(10043):505–517. - PubMed
-
- Sperling RA, Aisen PS, Beckett LA, Bennett DA, Craft S, Fagan AM, Iwatsubo T, Jack CR, Jr, Kaye J, Montine TJ, Park DC, Reiman EM, Rowe CC, Siemers E, Stern Y, Yaffe K, Carrillo MC, Thies B, Morrison-Bogorad M, Wagster MV, Phelps CH. Toward defining the preclinical stages of Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):280–292. - PMC - PubMed
-
- Jessen F, Amariglio RE, van Boxtel M, Breteler M, Ceccaldi M, Chételat G, Dubois B, Dufouil C, Ellis KA, van der Flier WM, Glodzik L, van Harten AC, de Leon MJ, McHugh P, Mielke MM, Molinuevo JL, Mosconi L, Osorio RS, Perrotin A, Petersen RC, Rabin LA, Rami L, Reisberg B, Rentz DM, Sachdev PS, de la Sayette V, Saykin AJ, Scheltens P, Shulman MB, Slavin MJ, Sperling RA, Stewart R, Uspenskaya O, Vellas B, Visser PJ, Wagner M, Subjective Cognitive Decline Initiative (SCD-I) Working Group A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement. 2014;10:844–852. - PMC - PubMed
-
- Jessen F, Wolfsgruber S, Wiese B, Bickel H, Mösch E, Kaduszkiewicz H, Pentzek M, Riedel-Heller SG, Luck T, Fuchs A, Weyerer S, Werle J, van den Bussche H, Scherer M, Maier W, Wagner M, German Study on Aging, Cognition and Dementia in Primary Care Patients AD dementia risk in late MCI, in early MCI, and in subjective memory impairment. Alzheimers Dement. 2014;10(1):76–83. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
