

The Relationship Between CGM-Derived Metrics, A1C, and Risk of Hypoglycemia in Older Adults With Type 1 Diabetes
- PMID: 32461211
- PMCID: PMC7510030
- DOI: 10.2337/dc20-0016
The Relationship Between CGM-Derived Metrics, A1C, and Risk of Hypoglycemia in Older Adults With Type 1 Diabetes
Erratum in
-
Erratum. The Relationship Between CGM-Derived Metrics, A1C, and Risk of Hypoglycemia in Older Adults With Type 1 Diabetes. Diabetes Care 2020;43:2349-2354.Diabetes Care. 2021 Jan;44(1):299. doi: 10.2337/dc21-er01b. Epub 2020 Nov 6. Diabetes Care. 2021. PMID: 33158951 Free PMC article. No abstract available.
Abstract
Objective: Continuous glucose monitoring (CGM) is now commonly used in the management of type 1 diabetes (T1D). The CGM-derived coefficient of variation (CV) measures glucose variability, and the glucose management indicator (GMI) measures mean glycemia (previously called estimated A1C). However, their relationship with laboratory-measured A1C and the risk of hypoglycemia in older adults with T1D is not well studied.
Research design and methods: In a single-center study, older adults (age ≥65 years) with T1D wore a CGM device for 14 days. The CV (%) and GMI were calculated, and A1C and clinical and demographic information were collected.
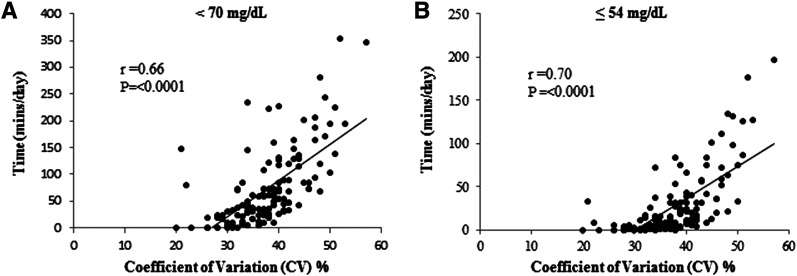
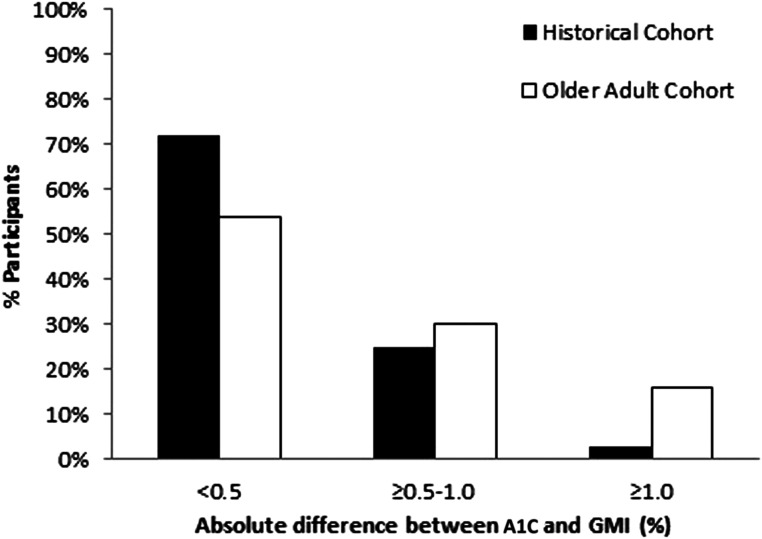
Results: We evaluated 130 older adults (age 71 ± 5 years), of whom 55% were women, 97% were White, diabetes duration was 39 ± 17 years, and A1C was 7.3 ± 0.6% (56 ± 15 mmol/mol). Participants were stratified by high CV (>36%; n = 77) and low CV (≤36%; n = 53). Although there was no difference in A1C levels between the groups with high and low CV (7.3% [56 mmol/mol] vs. 7.3% [53 mmol/mol], P = 0.4), the high CV group spent more time in hypoglycemia (<70 mg/dL and ≤54 mg/dL) compared with the group with low CV (median 31 vs. 84 min/day, P < 0.0001; 8 vs. 46 min/day, P < 0.001, respectively). An absolute difference between A1C and GMI of ≥0.5% was observed in 46% of the cohort. When the A1C was higher than the GMI by ≥0.5%, a higher duration of hypoglycemia was observed (P = 0.02).
Conclusions: In older adults with T1D, the use of CGM-derived CV and GMI can better identify individuals at higher risk for hypoglycemia compared with A1C alone. These measures should be combined with A1C for better diabetes management in older adults with T1D.
Trial registration: ClinicalTrials.gov NCT03078491.
© 2020 by the American Diabetes Association.
Figures
Comment in
-
Continuous Glucose Monitoring-Derived Data Report-Simply a Better Management Tool.Diabetes Care. 2020 Oct;43(10):2327-2329. doi: 10.2337/dci20-0032. Diabetes Care. 2020. PMID: 32958615 No abstract available.
Similar articles
-
Real-time CGM Is Superior to Flash Glucose Monitoring for Glucose Control in Type 1 Diabetes: The CORRIDA Randomized Controlled Trial.Diabetes Care. 2020 Nov;43(11):2744-2750. doi: 10.2337/dc20-0112. Epub 2020 Aug 28. Diabetes Care. 2020. PMID: 32859607 Free PMC article. Clinical Trial.
-
Effect of Continuous Glucose Monitoring on Hypoglycemia in Older Adults With Type 1 Diabetes: A Randomized Clinical Trial.JAMA. 2020 Jun 16;323(23):2397-2406. doi: 10.1001/jama.2020.6928. JAMA. 2020. PMID: 32543682 Free PMC article. Clinical Trial.
-
Intermittent-scanned continuous glucose monitoring with low glucose alarms decreases hypoglycemia incidence in middle-aged adults with type 1 diabetes in real-life setting.J Diabetes Complications. 2023 Feb;37(2):108385. doi: 10.1016/j.jdiacomp.2022.108385. Epub 2022 Dec 26. J Diabetes Complications. 2023. PMID: 36603333
-
Glucose Targets Using Continuous Glucose Monitoring Metrics in Older Adults With Diabetes: Are We There Yet?J Diabetes Sci Technol. 2024 Jul;18(4):808-818. doi: 10.1177/19322968241247568. Epub 2024 May 7. J Diabetes Sci Technol. 2024. PMID: 38715259 Free PMC article. Review.
-
Limitations of 14-Day Continuous Glucose Monitoring Sampling for Assessment of Hypoglycemia and Glycemic Variability in Type 1 Diabetes.Diabetes Technol Ther. 2024 Jul;26(7):503-508. doi: 10.1089/dia.2023.0476. Epub 2024 Feb 16. Diabetes Technol Ther. 2024. PMID: 38300516 Review.
Cited by
-
Usefulness of CGM-Derived Metric, the Glucose Management Indicator, to Assess Glycemic Control in Non-White Individuals With Diabetes.Diabetes Care. 2021 Dec;44(12):2787-2789. doi: 10.2337/dc21-1373. Epub 2021 Oct 11. Diabetes Care. 2021. PMID: 34635503 Free PMC article.
-
Association between the GMI/HbA1c ratio and preclinical carotid atherosclerosis in type 1 diabetes: impact of the fast-glycator phenotype across age groups.Cardiovasc Diabetol. 2025 Feb 14;24(1):75. doi: 10.1186/s12933-025-02637-4. Cardiovasc Diabetol. 2025. PMID: 39953520 Free PMC article.
-
Narrative Review: Continuous Glucose Monitoring (CGM) in Older Adults with Diabetes.Diabetes Ther. 2025 Jun;16(6):1139-1154. doi: 10.1007/s13300-025-01720-z. Epub 2025 Apr 16. Diabetes Ther. 2025. PMID: 40238078 Free PMC article. Review.
-
Ageing well with diabetes: the role of technology.Diabetologia. 2024 Oct;67(10):2085-2102. doi: 10.1007/s00125-024-06240-2. Epub 2024 Aug 13. Diabetologia. 2024. PMID: 39138689 Free PMC article. Review.
-
Dysglycemia in adults at risk for or living with non-insulin treated type 2 diabetes: Insights from continuous glucose monitoring.EClinicalMedicine. 2021 Apr 25;35:100853. doi: 10.1016/j.eclinm.2021.100853. eCollection 2021 May. EClinicalMedicine. 2021. PMID: 33997745 Free PMC article.
References
-
- Dhaliwal R, Foster NC, Boyle C, et al. . Determinants of fracture in adults with type 1 diabetes in the USA: results from the T1D exchange clinic registry. J Diabetes Complications 2018;32:1006–1011 - PubMed
-
- Lipska KJ, Kosiborod M. Hypoglycemia and adverse outcomes: marker or mediator? Rev Cardiovasc Med 2011;12:132–135 - PubMed
-
- Weinstock RS, DuBose SN, Bergenstal RM, et al. .; T1D Exchange Severe Hypoglycemia in Older Adults With Type 1 Diabetes Study Group . Risk factors associated with severe hypoglycemia in older adults with type 1 diabetes. Diabetes Care 2016;39:603–610 - PubMed
-
- Stahn A, Pistrosch F, Ganz X, et al. . Relationship between hypoglycemic episodes and ventricular arrhythmias in patients with type 2 diabetes and cardiovascular diseases: silent hypoglycemias and silent arrhythmias. Diabetes Care 2014;37:516–520 - PubMed
