

Invasive breast cancer and breast cancer mortality after ductal carcinoma in situ in women attending for breast screening in England, 1988-2014: population based observational cohort study
- PMID: 32461218
- PMCID: PMC7251423
- DOI: 10.1136/bmj.m1570
Invasive breast cancer and breast cancer mortality after ductal carcinoma in situ in women attending for breast screening in England, 1988-2014: population based observational cohort study
Abstract
Objective: To evaluate the long term risks of invasive breast cancer and death from breast cancer after ductal carcinoma in situ (DCIS) diagnosed through breast screening.
Design: Population based observational cohort study.
Setting: Data from the NHS Breast Screening Programme and the National Cancer Registration and Analysis Service.
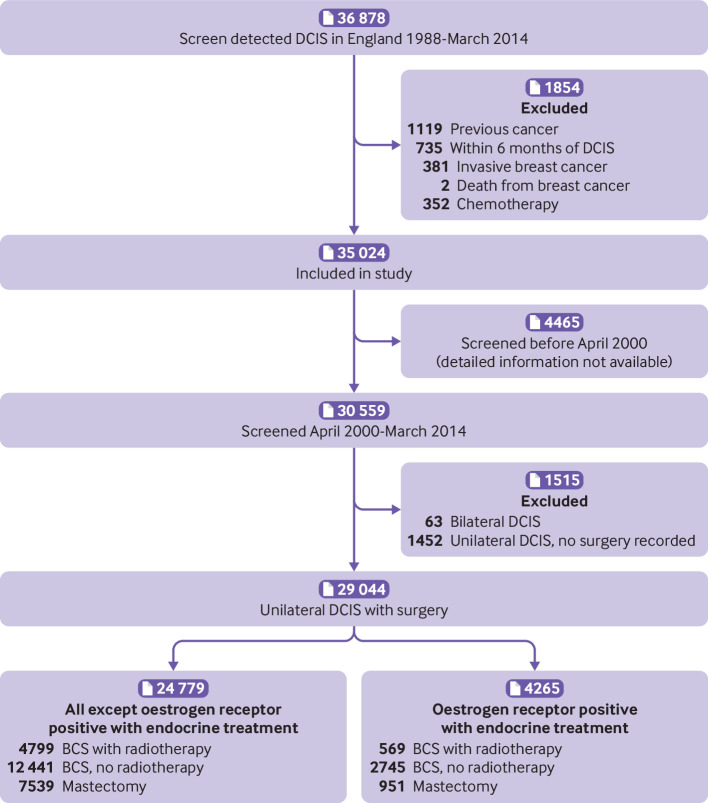
Participants: All 35 024 women in England diagnosed as having DCIS by the NHS Breast Screening Programme from its start in 1988 until March 2014.
Main outcome measures: Incident invasive breast cancer and death from breast cancer.
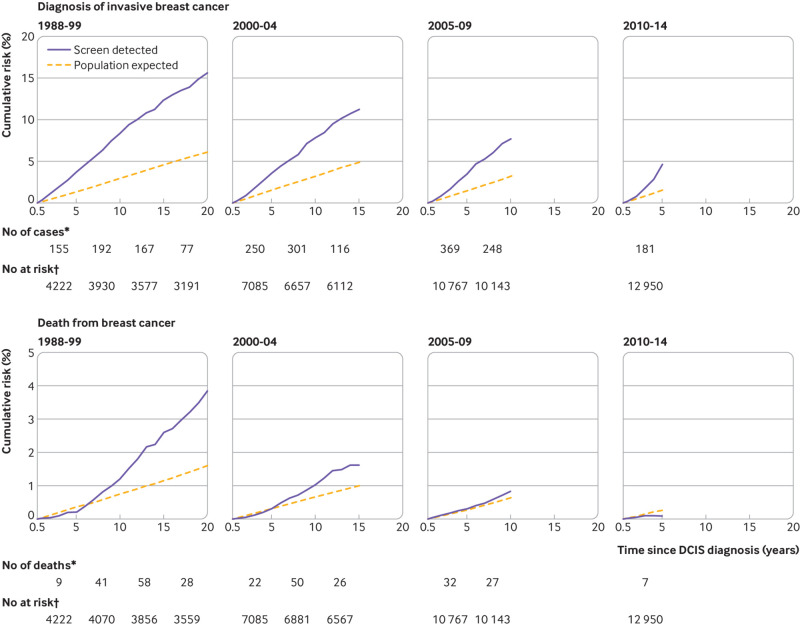
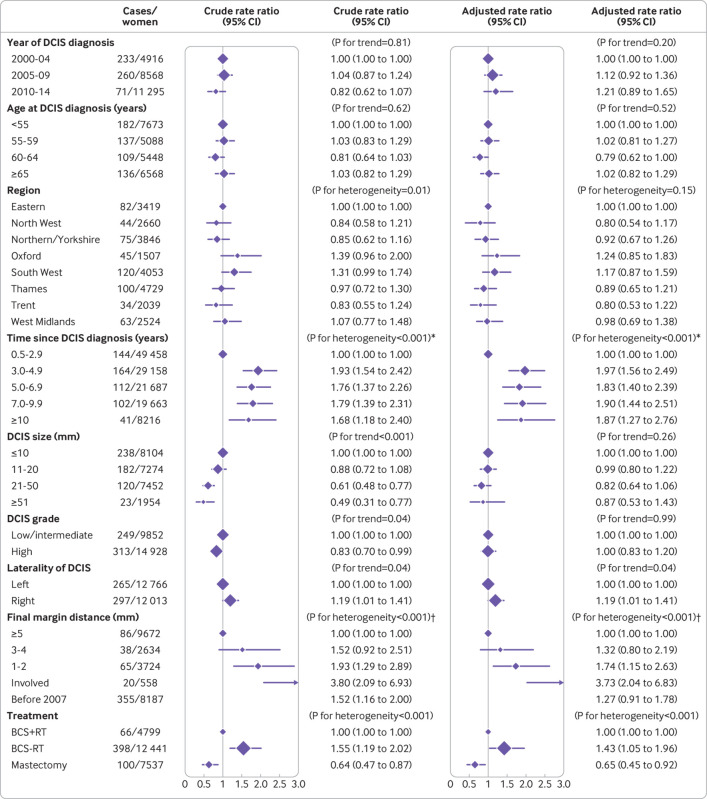
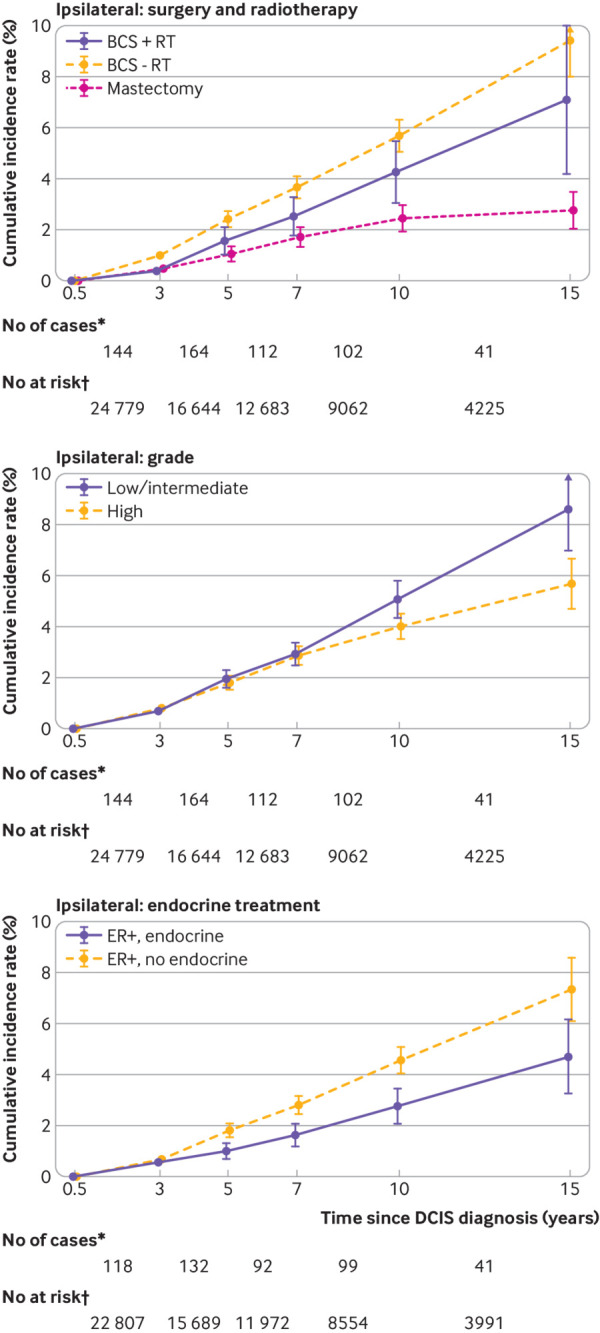
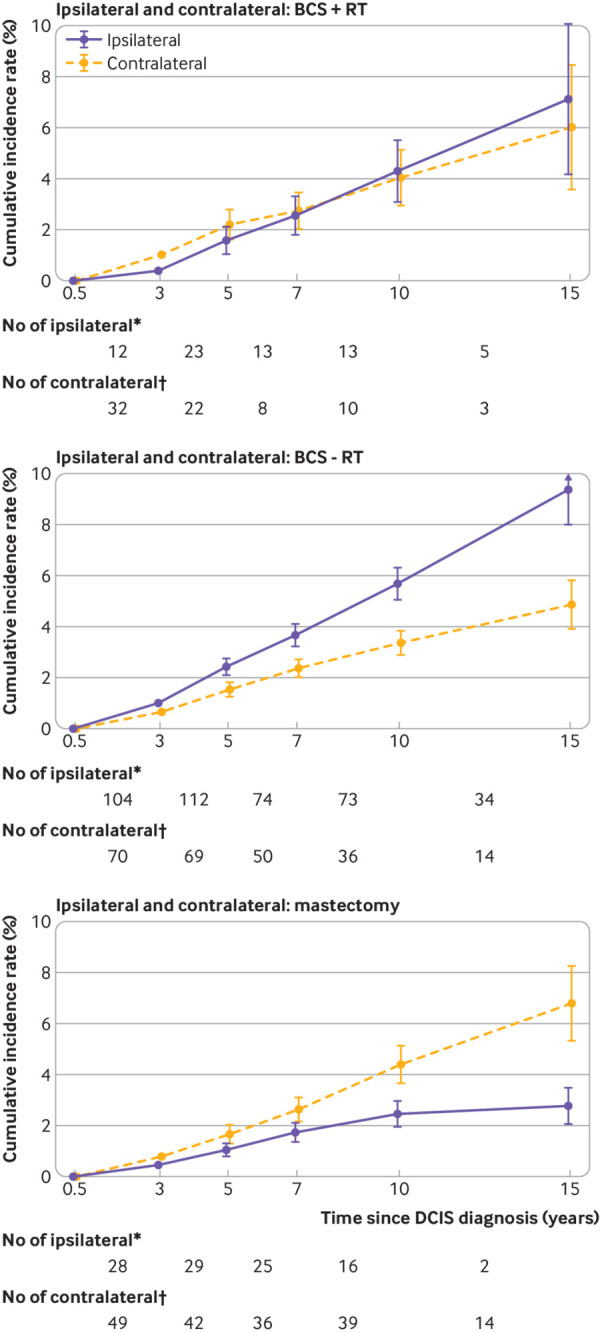
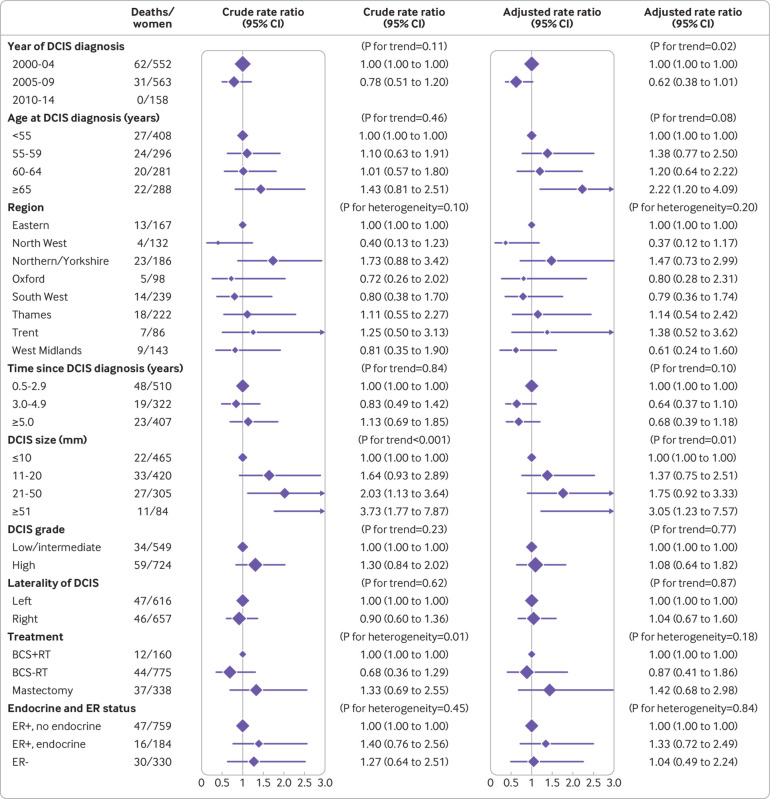
Results: By December 2014, 13 606 women had been followed for up to five years, 10 998 for five to nine years, 6861 for 10-14 years, 2620 for 15-19 years, and 939 for at least 20 years. Among these women, 2076 developed invasive breast cancer, corresponding to an incidence rate of 8.82 (95% confidence interval 8.45 to 9.21) per 1000 women per year and more than double that expected from national cancer incidence rates (ratio of observed rate to expected rate 2.52, 95% confidence interval 2.41 to 2.63). The increase started in the second year after diagnosis of DCIS and continued until the end of follow-up. In the same group of women, 310 died from breast cancer, corresponding to a death rate of 1.26 (1.13 to 1.41) per 1000 women per year and 70% higher than that expected from national breast cancer mortality rates (observed:expected ratio 1.70, 1.52 to 1.90). During the first five years after diagnosis of DCIS, the breast cancer death rate was similar to that expected from national mortality rates (observed:expected ratio 0.87, 0.69 to 1.10), but it then increased, with values of 1.98 (1.65 to 2.37), 2.99 (2.41 to 3.70), and 2.77 (2.01 to 3.80) in years five to nine, 10-14, and 15 or more after DCIS diagnosis. Among 29 044 women with unilateral DCIS undergoing surgery, those who had more intensive treatment (mastectomy, radiotherapy for women who had breast conserving surgery, and endocrine treatment in oestrogen receptor positive disease) and those with larger final surgical margins had lower rates of invasive breast cancer.
Conclusions: To date, women with DCIS detected by screening have, on average, experienced higher long term risks of invasive breast cancer and death from breast cancer than women in the general population during a period of at least two decades after their diagnosis. More intensive treatment and larger final surgical margins were associated with lower risks of invasive breast cancer.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from Cancer Research UK, the National Institute for Health Research Biomedical Research Centre, and the UK Medical Research Council for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; and no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Youngwirth LM, Boughey JC, Hwang ES. Surgery versus monitoring and endocrine therapy for low-risk DCIS: The COMET Trial. Bull Am Coll Surg 2017;102:62-3. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical