

Contactin-1 autoimmunity: Serologic, neurologic, and pathologic correlates
- PMID: 32461352
- PMCID: PMC7286654
- DOI: 10.1212/NXI.0000000000000771
Contactin-1 autoimmunity: Serologic, neurologic, and pathologic correlates
Abstract
Objective: To determine serologic characteristics, frequency, phenotype, paraneoplastic associations, and electrodiagnostic and histopathologic features accompanying contactin-1 autoimmunity.
Methods: Archived sera known to produce synaptic tissue-based immunofluorescence patterns were reevaluated, and contactin-1 specificity was confirmed by recombinant protein assays. Screening of 233 chronic/relapsing demyelinating neuropathies for additional cases was performed.
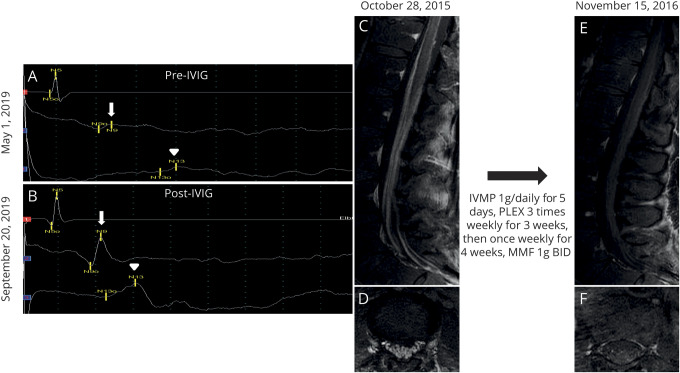
Results: We identified 10 contactin-1 IgG seropositive cases. Frequency of contactin-1 immunoglobulin (Ig) G among tested Mayo Clinic chronic/relapsing demyelinating neuropathies was 2%. Sensory predominant presentations (n = 9, 90%), neuropathic pain (n = 6, 60%), and subacute progression (n = 5, 50%) were commonly encountered among contactin-1 neuropathies. Two patients had chronic immune sensory polyradiculopathy-like phenotype at presentation. Electrodiagnostic studies were consistent with demyelination (slowed conduction velocities and/or prolonged distal latencies) without conduction block. Markedly elevated CSF protein (median 222 mg/dL, range 69-960 mg/dL), thickening/gadolinium enhancement of nerve roots (4/5), and subperineural edema on nerve biopsy (4/4) were other characteristic features. Three cases were diagnosed with paraneoplastic demyelinating neuropathies (thymoma, n = 1; breast cancer, n = 1; plasmacytoma, n = 1). Four of the 9 patients treated with IV immunoglobulin demonstrated initial clinical improvement, but the favorable response was sustained in only 1 case (median follow-up, 60 months). Sustained clinical stabilization or improvement was observed among 3 of the 6 cases in whom second-line therapies (rituximab, cyclophosphamide, and azathioprine) were used.
Conclusion: Contactin-1 IgG has a distinct sensory predominant presentation commonly associated with neuropathic pain, with demyelinating changes on electrophysiologic studies. A paraneoplastic cause should be considered. Testing of contactin-1 IgG among cases with similar presentations may guide immunotherapy selection, especially second-line immunotherapy consideration.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures

References
-
- Querol L, Devaux J, Rojas-Garcia R, Illa I. Autoantibodies in chronic inflammatory neuropathies: diagnostic and therapeutic implications. Nat Rev Neurol 2017;13:533–547. - PubMed
-
- Doppler K, Appeltshauser L, Wilhelmi K, et al. . Destruction of paranodal architecture in inflammatory neuropathy with anti-contactin-1 autoantibodies. J Neurol Neurosurg Psychiatry 2015;86:720–728. - PubMed
-
- Querol L, Nogales-Gadea G, Rojas-Garcia R, et al. . Antibodies to contactin-1 in chronic inflammatory demyelinating polyneuropathy. Ann Neurol 2013;73:370–380. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous