

Photoacoustic imaging for three-dimensional visualization and delineation of basal cell carcinoma in patients
- PMID: 32461885
- PMCID: PMC7243191
- DOI: 10.1016/j.pacs.2020.100187
Photoacoustic imaging for three-dimensional visualization and delineation of basal cell carcinoma in patients
Abstract
Background: Photoacoustic (PA) imaging is an emerging non-invasive biomedical imaging modality that could potentially be used to determine the borders of basal cell carcinomas (BCC) preoperatively in order to reduce the need for repeated surgery.
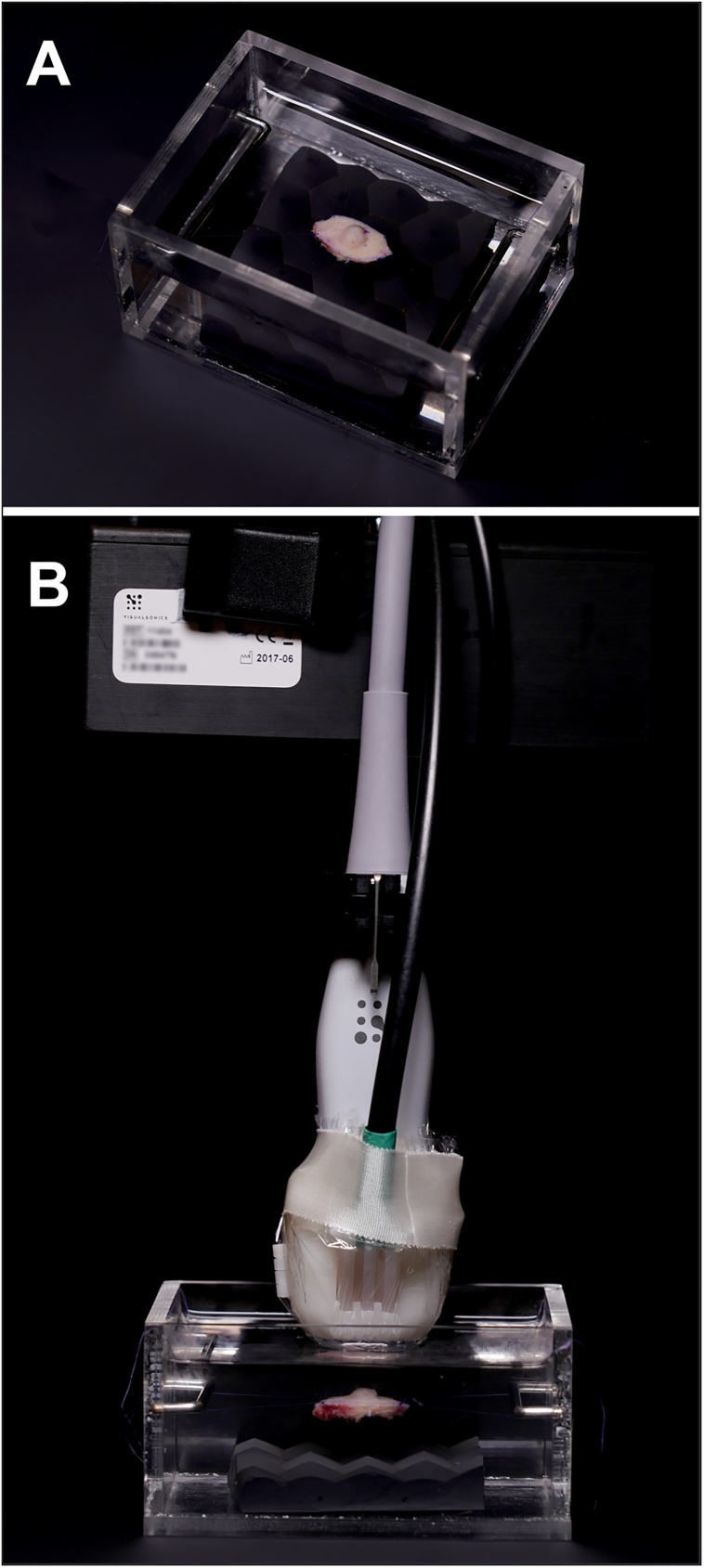
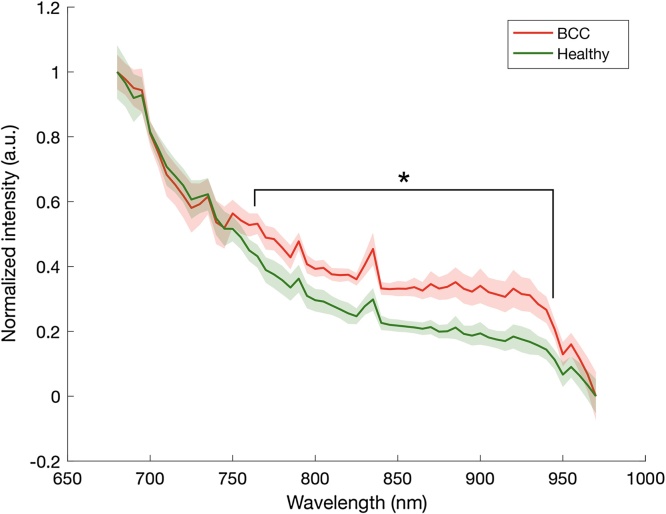
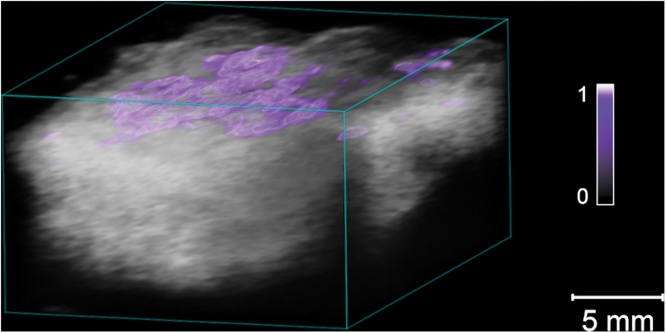
Methods: Two- and three-dimensional PA images were obtained by scanning BCCs using 59 wavelengths in the range 680-970 nm. Spectral unmixing was performed to visualize the tumor tissue distribution. Spectral signatures from 38 BCCs and healthy tissue were compared ex vivo.
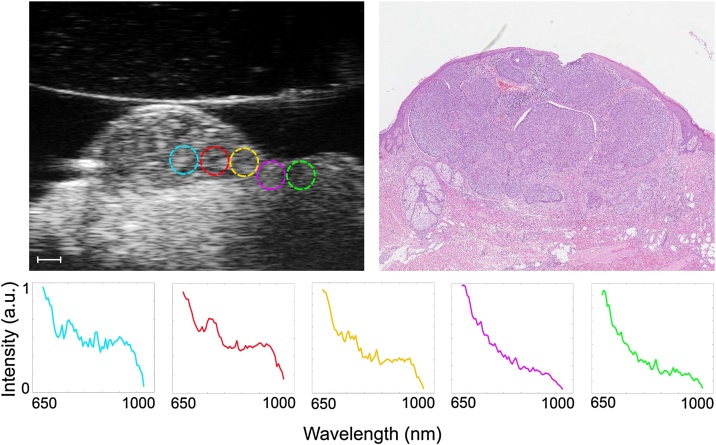
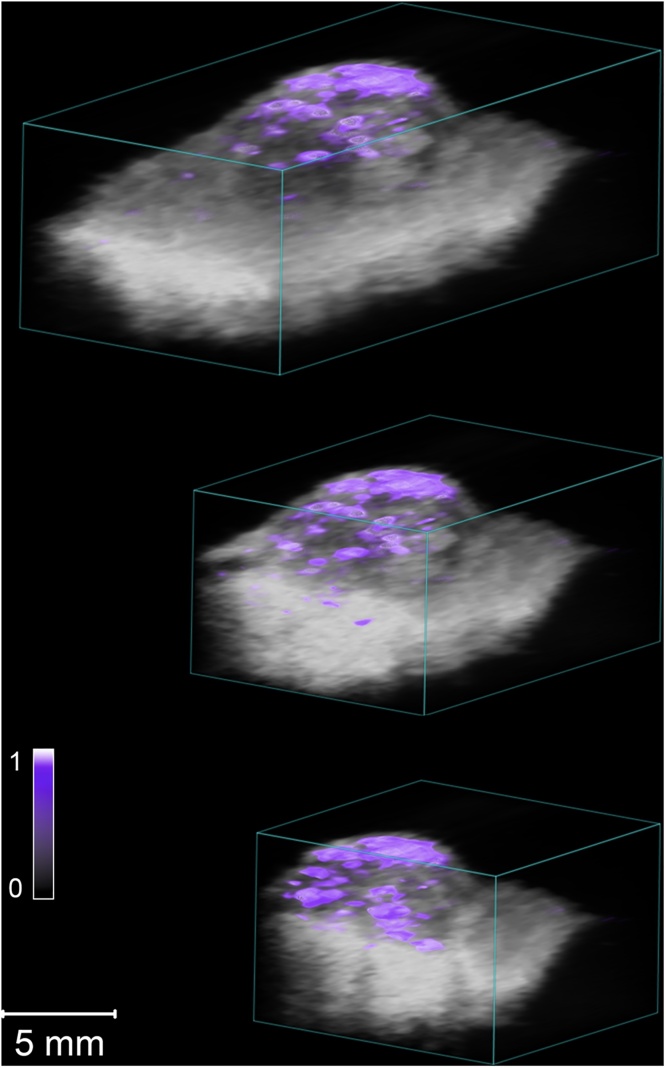
Results and discussion: The PA spectra could be used to differentiate between BCC and healthy tissue ex vivo (p < 0.05). Spectral unmixing provided visualization of the overall architecture of the lesion and its border.
Conclusion: PA imaging can be used to differentiate between BCC and healthy tissue and can potentially be used to delineate tumors prior to surgical excision.
Keywords: Basal cell carcinoma; Basalioma; Human; Patients; Photoacoustic imaging; Spectral unmixing; Tissue differentiation.
© 2020 The Author(s).
Conflict of interest statement
A conflicting interest exists when professional judgement concerning a primary interest (such as patient’s welfare or the validity of research) may be influenced by a secondary interest (such as financial gain or personal rivalry). It may arise for the authors when they have financial interest that may influence their interpretation of their results or those of others. Examples of potential conflicts of interest include employment, consultancies, stock ownership, honoraria, paid expert testimony, patent applications/registrations, and grants or other funding.
Figures
References
-
- Lomas A., Leonardi-Bee J., Bath-Hextall F. A systematic review of worldwide incidence of nonmelanoma skin cancer. Br. J. Dermatol. 2012;166(5):1069–1080. - PubMed
-
- Cameron M.C., Lee E., Hibler B., Barker C.A., Mori S., Cordova M., Nehal K.S., Rossi A.M. Basal cell carcinoma: part 1. J. Am. Acad. Dermatol. 2018 - PubMed
-
- Lewis K.G., Weinstock M.A. Nonmelanoma skin cancer mortality (1988–2000): the Rhode island follow-back study. Arch. Dermatol. 2004;140(7):837–842. - PubMed
-
- Thomas D.J., King A.R., Peat B.G. Excision margins for nonmelanotic skin cancer. Plast. Reconstr. Surg. 2003;112(1):57–63. - PubMed
LinkOut - more resources
Full Text Sources
