

The Safety and Feasibility of Enhanced Recovery after Surgery in Patients Undergoing Pancreaticoduodenectomy: An Updated Meta-Analysis
- PMID: 32462014
- PMCID: PMC7232716
- DOI: 10.1155/2020/7401276
The Safety and Feasibility of Enhanced Recovery after Surgery in Patients Undergoing Pancreaticoduodenectomy: An Updated Meta-Analysis
Abstract
Background: Enhanced recovery after surgery (ERAS) is a multimodal, multidisciplinary, evidence-based approach to care for surgical patients and aims at optimizing the perioperative management and outcomes. The ERAS approach was first implemented in colorectal surgery patients; however, the reported applications in pancreatoduodenectomy patients are limited. In recent years, studies on ERAS for patients undergoing pancreaticoduodenectomy have been published. The accumulation of new randomized controlled trials and high-quality case-control studies stimulated us to update the analysis. Our study comprehensively collected data to provide the best evidence summary for the clinic.
Aim: To evaluate the safety and feasibility of enhanced recovery after surgery in the perioperative management of pancreatoduodenectomy patients.
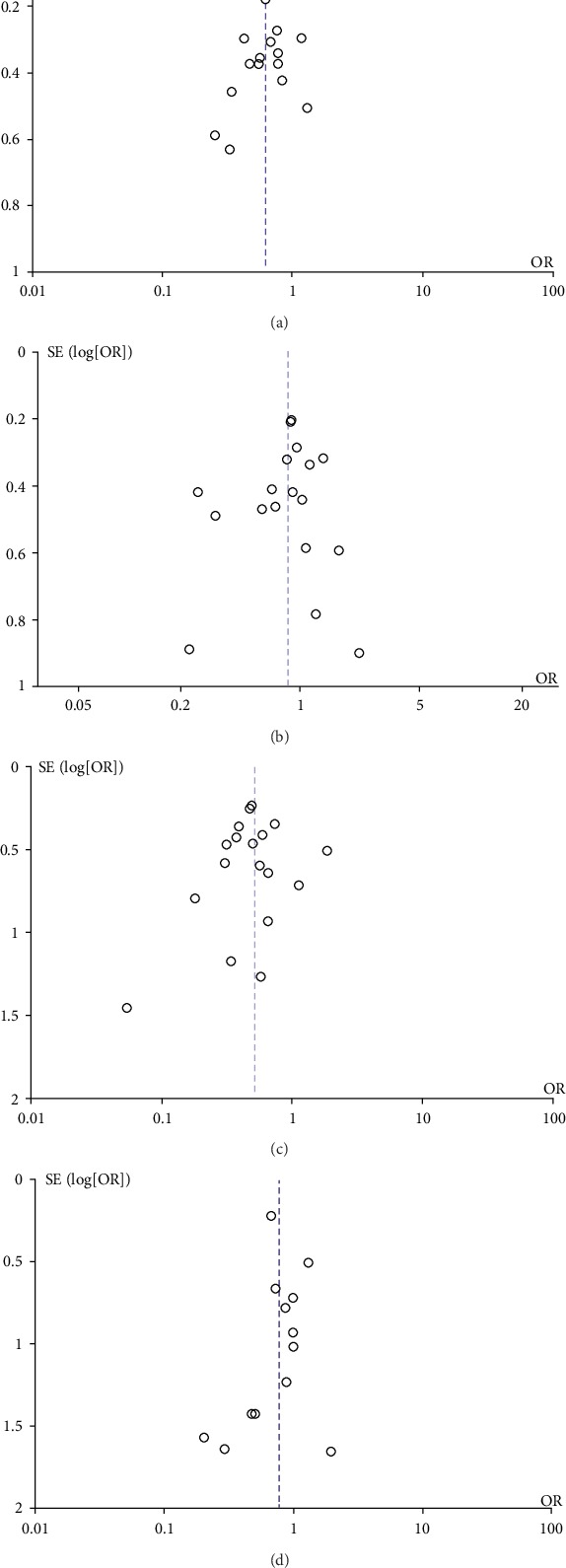
Methods: A systematic literature search of PubMed, Embase, and the Cochrane Library was performed up to July 2019. All randomized controlled trials and case-control studies that applied ERAS for patients undergoing pancreaticoduodenectomy were considered for inclusion in this study. The patients were divided into two groups: patients who received the ERAS perioperative management approach were defined as the ERAS group and patients who received the traditional perioperative management approach were defined as the control group. All statistical analyses were conducted using the Revman5.3 software, and the outcomes were calculated as odds ratios or weighted mean differences with their corresponding 95% confidence intervals. A funnel plot was created to assess publication bias. Subgroup and sensitivity analyses were performed to explore the sources of heterogeneity.
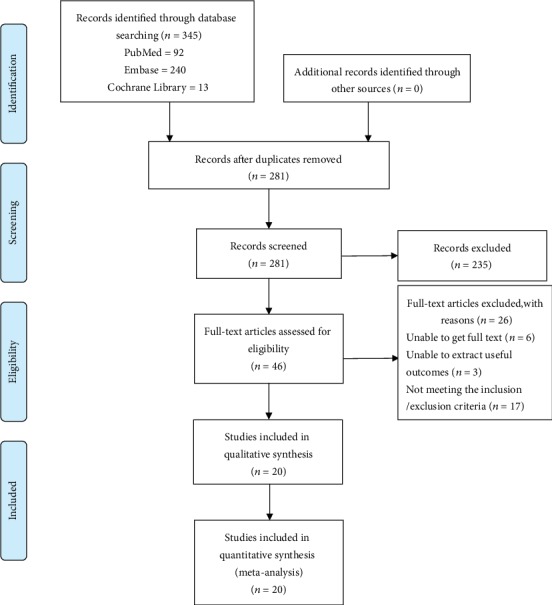
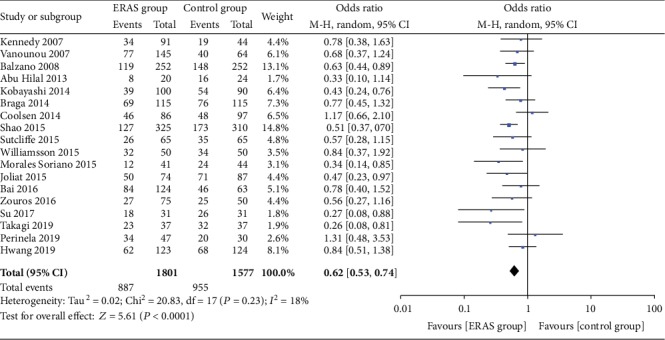
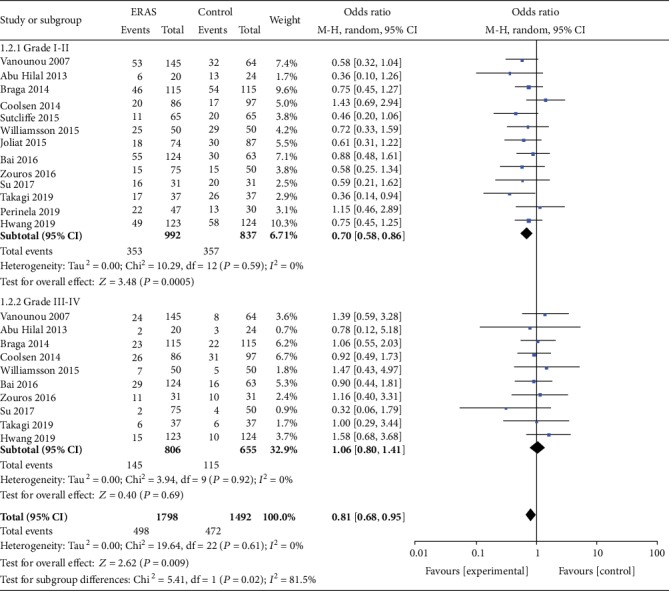
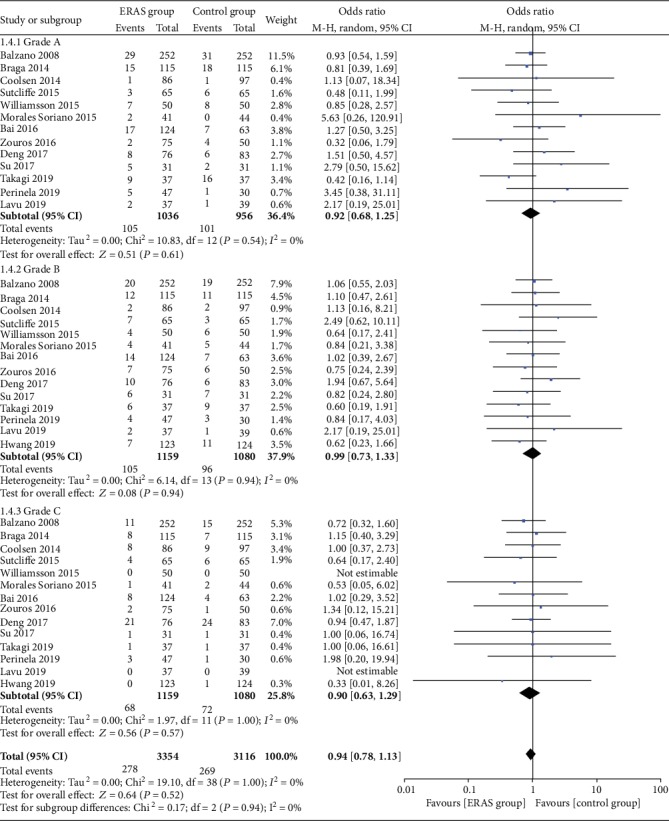
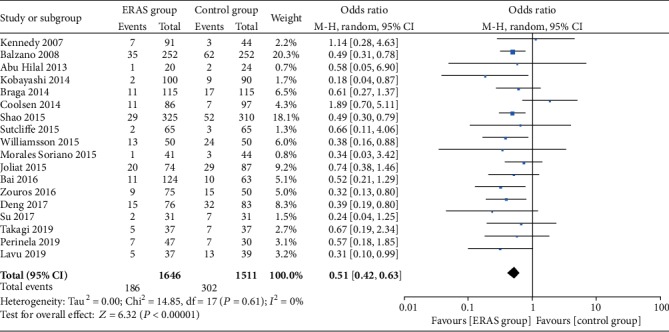
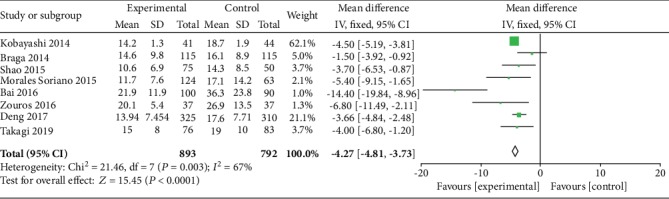
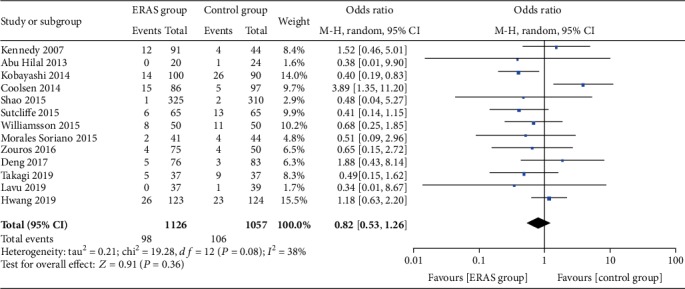
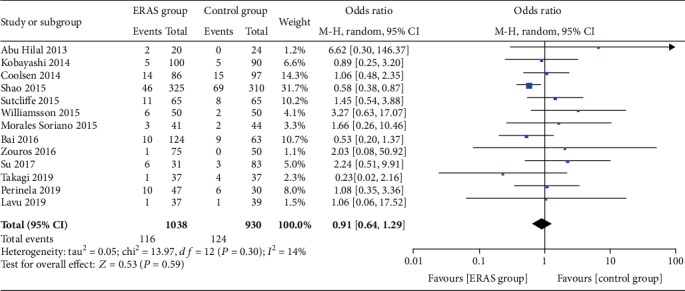
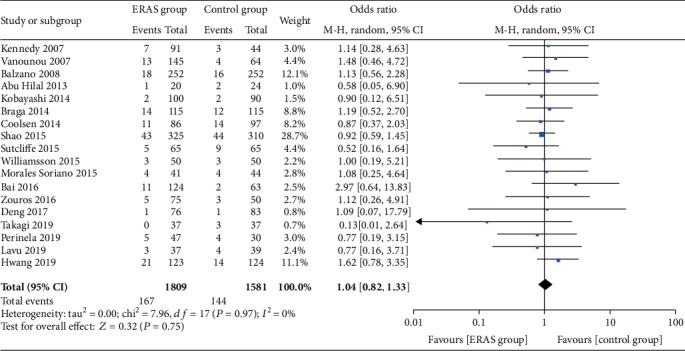
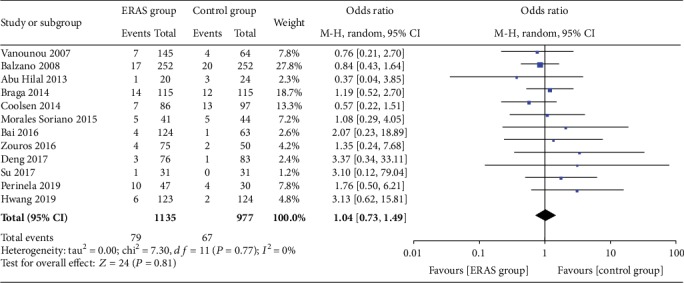
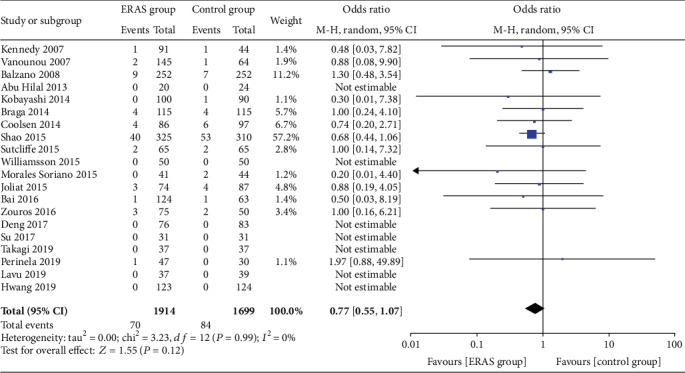
Results: A total of 20 studies involving 3613 patients (1914 patients in the ERAS group vs. 1699 patients in the control group) were included in this study. Among the 20 studies, 4 were randomized controlled trials, and 16 were case-control studies. The overall postoperative complication rate was significantly lower in the ERAS group (OR = 0.62, 95% CI: 0.53-0.74, P < 0.00001) than in the control group. In addition, the minor complication rate (Clavien-Dindo I-II) was also lower in the ERAS group (OR = 0.70, 95% CI: 0.58-0.86, P = 0.0005). The patients in the ERAS group had a lower incidence of delayed gastric emptying (OR = 0.51, 95% CI: 0.42-0.63, P < 0.00001) and shorter length of hospital stay (WMD = -4.27, 95% CI: -4.81~-3.73, P < 0.00001) than in the control group. The rates of pancreatic fistula (regardless of Grade A/B/C), wound infections, abdominal abscesses, readmission, reoperation, and morbidity were not significantly different between the two groups.
Conclusion: The ERAS approach is safe and effective in the perioperative management of patients undergoing pancreaticoduodenectomy and helps to accelerate the postoperative recovery and improve prognosis.
Copyright © 2020 You-Meng Sun et al.
Conflict of interest statement
There are no conflicts of interest associated with any of authors of this manuscript.
Figures
Similar articles
-
Impact of enhanced recovery after surgery programs on pancreatic surgery: A meta-analysis.World J Gastroenterol. 2018 Apr 21;24(15):1666-1678. doi: 10.3748/wjg.v24.i15.1666. World J Gastroenterol. 2018. PMID: 29686474 Free PMC article.
-
Reducing postoperative complications and improving clinical outcome: Enhanced recovery after surgery in pancreaticoduodenectomy - A retrospective cohort study.Int J Surg. 2017 Mar;39:176-181. doi: 10.1016/j.ijsu.2017.01.089. Epub 2017 Jan 26. Int J Surg. 2017. PMID: 28132917
-
Is total laparoscopic pancreaticoduodenectomy superior to open procedure? A meta-analysis.World J Gastroenterol. 2019 Oct 7;25(37):5711-5731. doi: 10.3748/wjg.v25.i37.5711. World J Gastroenterol. 2019. PMID: 31602170 Free PMC article.
-
[Safety of enhanced recovery after surgery (ERAS) protocol in the treatment of patients undergoing pancreatoduodenectomy].Khirurgiia (Mosk). 2021;(11):19-26. doi: 10.17116/hirurgia202111119. Khirurgiia (Mosk). 2021. PMID: 34786912 Russian.
-
Impact of enhanced recovery after surgery protocol on pancreaticoduodenectomy: a meta-analysis of non-randomized and randomized controlled trials.HPB (Oxford). 2020 Oct;22(10):1373-1383. doi: 10.1016/j.hpb.2020.07.001. Epub 2020 Aug 15. HPB (Oxford). 2020. PMID: 32811766 Review.
Cited by
-
Complications after Supramajor Gastrointestinal Surgery: Role of Enhanced Recovery after Surgery.Indian J Crit Care Med. 2020 Sep;24(Suppl 4):S205-S210. doi: 10.5005/jp-journals-10071-23615. Indian J Crit Care Med. 2020. PMID: 33354043 Free PMC article. Review.
-
Costs and clinical benefits of enhanced recovery after surgery (ERAS) in pancreaticoduodenectomy: an updated systematic review and meta-analysis.J Cancer Res Clin Oncol. 2023 Aug;149(9):6639-6660. doi: 10.1007/s00432-022-04508-x. Epub 2023 Jan 11. J Cancer Res Clin Oncol. 2023. PMID: 36629919 Free PMC article.
-
A Scientometric Analysis and Visualization Discovery of Enhanced Recovery After Surgery.Front Surg. 2022 Jun 8;9:894083. doi: 10.3389/fsurg.2022.894083. eCollection 2022. Front Surg. 2022. PMID: 36090333 Free PMC article.
-
Optimized perioperative management (fast-track, ERAS) to enhance postoperative recovery in elective colorectal surgery.GMS Hyg Infect Control. 2022 Jun 23;17:Doc10. doi: 10.3205/dgkh000413. eCollection 2022. GMS Hyg Infect Control. 2022. PMID: 35909653 Free PMC article. Review.
-
Associations Between Patient Characteristics and Whipple Procedure Outcomes Before and After Implementation of an Enhanced Recovery After Surgery Protocol.J Gastrointest Surg. 2023 Sep;27(9):1855-1866. doi: 10.1007/s11605-023-05693-x. Epub 2023 May 10. J Gastrointest Surg. 2023. PMID: 37165160
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
