

Analysis of Lumbar Sagittal Curvature in Spinal Decompression and Fusion for Lumbar Spinal Stenosis Patients under Roussouly Classification
- PMID: 32462019
- PMCID: PMC7222496
- DOI: 10.1155/2020/8078641
Analysis of Lumbar Sagittal Curvature in Spinal Decompression and Fusion for Lumbar Spinal Stenosis Patients under Roussouly Classification
Abstract
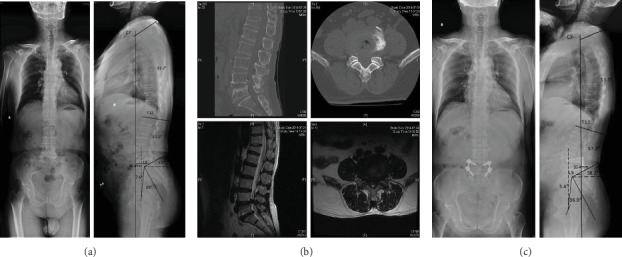
To evaluate the clinical significance of spinal decompression and fusion for lumbar spinal stenosis in old patients under Roussouly classification, 160 old patients (>60 year old) with lumbar spinal stenosis underwent spinal decompression, and fusion were retrospectively studied. According to Roussouly classification, patients were divided into 4 groups, in which Roussouly types I, II, and IV were the nonstandard group and Roussouly type III was the standard group. Visual analog scale (waist, leg) and Oswestry disability index (ODI) scores were recorded before operation and at the final follow-up. All patients improved the sagittal curvature: for patients in Roussouly types I and II, there were statistically significant differences in terms of postoperative global lordosis (GL), global kyphosis (GK), sacral slope (SS), sagittal vertical axis (SVA), and pelvic tilt (PT) compared with that before surgery (all P < 0.001); patients in Roussouly type IV obtained similar results with type III after surgery. The four groups showed significant improvement in ODI and VAS scores at final follow-up (all P < 0.001). After regrouping at the final follow-up, the proportion of the standard type (Roussouly type III) patients was increased compared with preoperative. In conclusion, Roussouly classification has important guiding significance in spinal decompression and fusion for old patients (>60 years) with lumbar spinal stenosis.
Copyright © 2020 Guoqiang Zhang et al.
Conflict of interest statement
The authors declare that there is no conflict of interest regarding the publication of this paper.
Figures



Similar articles
-
The sagittal spinal profile type: a principal precondition for surgical decision making in patients with lumbar spinal stenosis.J Neurosurg Spine. 2017 Nov;27(5):552-559. doi: 10.3171/2017.3.SPINE161269. Epub 2017 Sep 1. J Neurosurg Spine. 2017. PMID: 28862573
-
Characterization of Sagittal Spine Alignment With Reference to the Gravity Line and Vertebral Slopes: An Analysis of Different Roussouly Curves.Spine (Phila Pa 1976). 2020 May 1;45(9):E481-E488. doi: 10.1097/BRS.0000000000003379. Spine (Phila Pa 1976). 2020. PMID: 32282653
-
Short Lumbosacral Decompression Plus Fixation Does Not Change the Spinopelvic Balance on Patients With Moderate Degenerative Spondylolisthesis and Associated Spinal Stenosis.Spine Deform. 2019 Mar;7(2):346-355. doi: 10.1016/j.jspd.2018.08.016. Spine Deform. 2019. PMID: 30660232
-
The Analysis of Preoperative Roussouly Classification on Pain Scores and Radiological Data in Lateral Lumbar Interbody Fusion for Patients with Lumbar Degenerative Disease.World Neurosurg. 2023 Jul;175:e380-e390. doi: 10.1016/j.wneu.2023.03.102. Epub 2023 Mar 30. World Neurosurg. 2023. PMID: 37003531
-
Comparison Between Fusion and Non-Fusion Surgery for Lumbar Spinal Stenosis: A Meta-analysis.Adv Ther. 2021 Mar;38(3):1404-1414. doi: 10.1007/s12325-020-01604-7. Epub 2021 Jan 24. Adv Ther. 2021. PMID: 33491158 Review.
Cited by
-
To Align Multimodal Lumbar Spine Images via Bending Energy Constrained Normalized Mutual Information.Biomed Res Int. 2020 Jul 10;2020:5615371. doi: 10.1155/2020/5615371. eCollection 2020. Biomed Res Int. 2020. PMID: 32733945 Free PMC article.
-
Influence of Lumbar Lordosis on Posterior Rod Strain in Long-Segment Construct During Biomechanical Loading: A Cadaveric Study.Neurospine. 2021 Sep;18(3):635-643. doi: 10.14245/ns.2142368.184. Epub 2021 Sep 30. Neurospine. 2021. PMID: 34610695 Free PMC article.
References
-
- Dubousset J. Importance de la vertèbre pelvienne dans l'équilibre rachidien. Application à la chirurgie de la colonne vertébrale chez l'enfant et l'adolescent. Pied équilibre et rachis; 1998.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
