

Risk of acute brain lesions in dizzy patients presenting to the emergency room: who needs imaging and who does not?
- PMID: 32462345
- PMCID: PMC7718179
- DOI: 10.1007/s00415-020-09909-x
Risk of acute brain lesions in dizzy patients presenting to the emergency room: who needs imaging and who does not?
Abstract
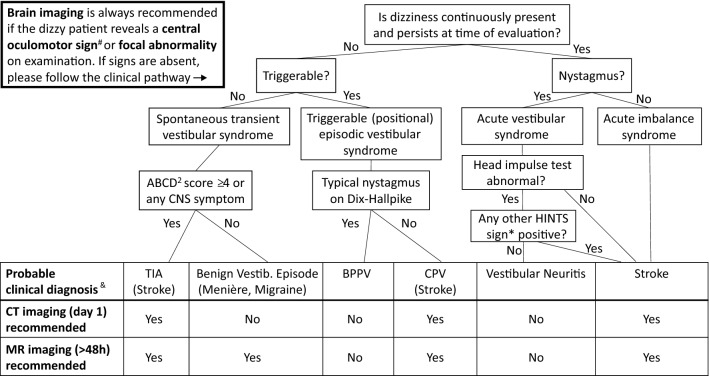
The usefulness of brain imaging studies in dizzy patients presenting to the emergency department (ED) is controversial. We aimed to assess the 'real-world' probability of ischemic stroke and other acute brain lesions (ABLs) in these patients to create an algorithm that helps decision-making on whether which and when brain imaging is needed. By reviewing medical records, we identified 610 patients presenting with dizziness, vertigo or imbalance to our university hospital's ED and receiving neurological workup. We collected timing/triggers of symptoms, ABCD2 score, focal neurological abnormalities, HINTS (head impulse, nystagmus, test-of-skew) and other central oculomotor signs. ABLs were extracted from CT/MRI reports. Uni-/multivariate logistic regression analyses investigated associations between clinical parameters and ABLs. Finally, the likelihood of ABLs was assessed for different clinically defined subgroups ('dizziness syndromes'). Early CT (day 1) was performed in 539 (88%) and delayed MR imaging (median: day 4) in 299 (49%) patients. ABLs (89% ischemic stroke) were revealed in 75 (24%) of 318 patients with adequate imaging (MRI or lesion-positive CT). The risk for ABLs increased with the presence of central oculomotor signs (odds ratio 2.8, 95% confidence interval 1.5-5.2) or focal abnormalities (OR 3.3, 95% CI 1.8-6.2). The likelihood of ABLs differed between dizziness syndromes, e.g., HINTS-negative acute vestibular syndrome: 0%, acute imbalance syndrome with ABCD2-score ≥ 4: 50%. We propose a clinical pathway, according to which patients with HINTS-negative acute vestibular syndrome should not receive brain imaging, whereas imaging is suggested in dizzy patients with acute imbalance, central oculomotor signs or focal abnormalities.
Keywords: CT; Dizziness; MRI; Nystagmus; Stroke; Vertigo.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

References
-
- Chalela JA, Kidwell CS, Nentwich LM, Luby M, Butman JA, Demchuk AM, Hill MD, Patronas N, Latour L, Warach S. Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison. Lancet. 2007;369:293–298. doi: 10.1016/S0140-6736(07)60151-2. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
