

Acute Symptomatic Seizures in Critically Ill Patients with COVID-19: Is There an Association?
- PMID: 32462412
- PMCID: PMC7253233
- DOI: 10.1007/s12028-020-01006-1
Acute Symptomatic Seizures in Critically Ill Patients with COVID-19: Is There an Association?
Abstract
Background: The coronavirus disease of 2019 (COVID-19) emerged as a global pandemic. Historically, the group of human coronaviruses can also affect the central nervous system leading to neurological symptoms; however, the causative mechanisms of the neurological manifestations of COVID-19 disease are not well known. Seizures have not been directly reported as a part of COVID-19 outside of patients with previously known brain injury or epilepsy. We report two cases of acute symptomatic seizures, in non-epileptic patients, associated with severe COVID-19 disease.
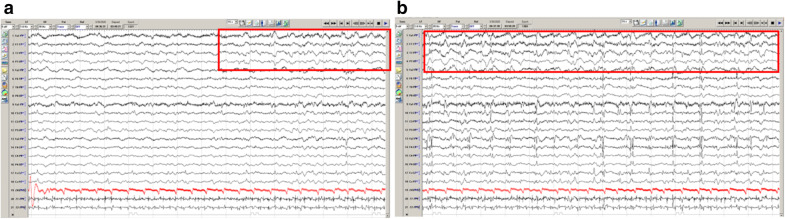
Case presentations: Two advanced-age, non-epileptic, male patients presented to our northeast Ohio-based health system with concern for infection in Mid-March 2020. Both had a history of lung disease and during their hospitalization tested positive for SARS-CoV-2. They developed acute encephalopathy days into their hospitalization with clinical and electrographic seizures. Resolution of seizures was achieved with levetiracetam.
Discussion: Patients with COVID-19 disease are at an elevated risk for seizures, and the mechanism of these seizures is likely multifactorial. Clinical (motor) seizures may not be readily detected in this population due to the expansive utilization of sedatives and paralytics for respiratory optimization strategies. Many of these patients are also not electrographically monitored for seizures due to limited resources, multifactorial risk for acute encephalopathy, and the risk of cross-contamination. Previously, several neurological symptoms were seen in patients with more advanced COVID-19 disease, and these were thought to be secondary to multi-system organ failure and/or disseminated intravascular coagulopathy-related brain injury. However, these patients may also have an advanced breakdown of the blood-brain barrier precipitated by pro-inflammatory cytokine reactions. The neurotropic effect and neuroinvasiveness of SARS-Coronavirus-2 have not been directly established.
Conclusions: Acute symptomatic seizures are possible in patients with COVID-19 disease. These seizures are likely multifactorial in origin, including cortical irritation due to blood-brain barrier breakdown, precipitated by the cytokine reaction as a part of the viral infection. Patients with clinical signs of seizures or otherwise unexplained encephalopathy may benefit from electroencephalography monitoring and/or empiric anti-epileptic therapy. Further studies are needed to elucidate the risk of seizures and benefit of monitoring in this population.
Keywords: Coronavirus; Seizures; Status epilepticus.
Conflict of interest statement
None of the authors listed have received any financial support for this manuscript and have no conflicts of interest to disclose.
Figures


References
-
- Mao L, Wang M, Chen S. Neurological manifestations of hospitalized patients with COVID-19 in Wuhan, China: a retrospective case series study. SSRN Electron J. 2020 doi: 10.2139/ssrn.3544840. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
