

Testicular tumours in children: an approach to diagnosis and management with pathologic correlation
- PMID: 32462465
- PMCID: PMC7253550
- DOI: 10.1186/s13244-020-00867-6
Testicular tumours in children: an approach to diagnosis and management with pathologic correlation
Abstract
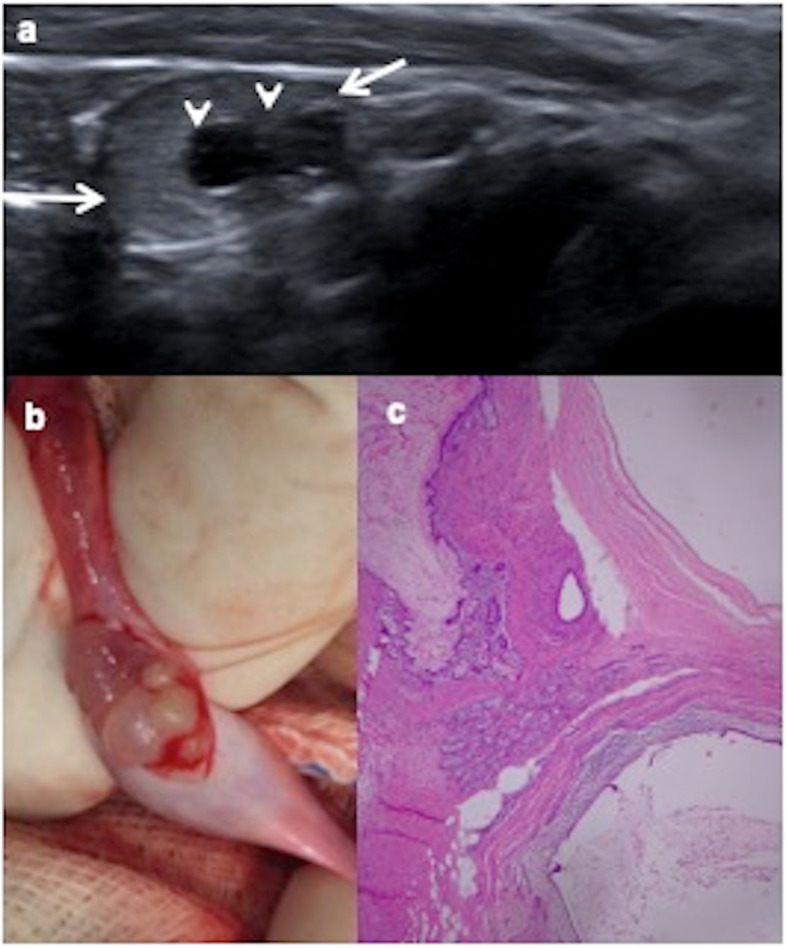
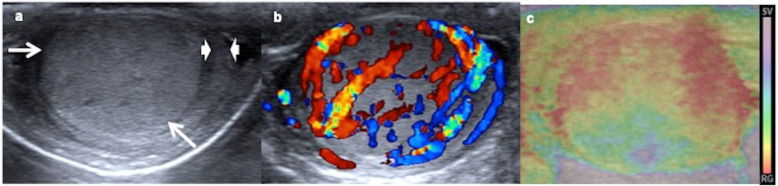
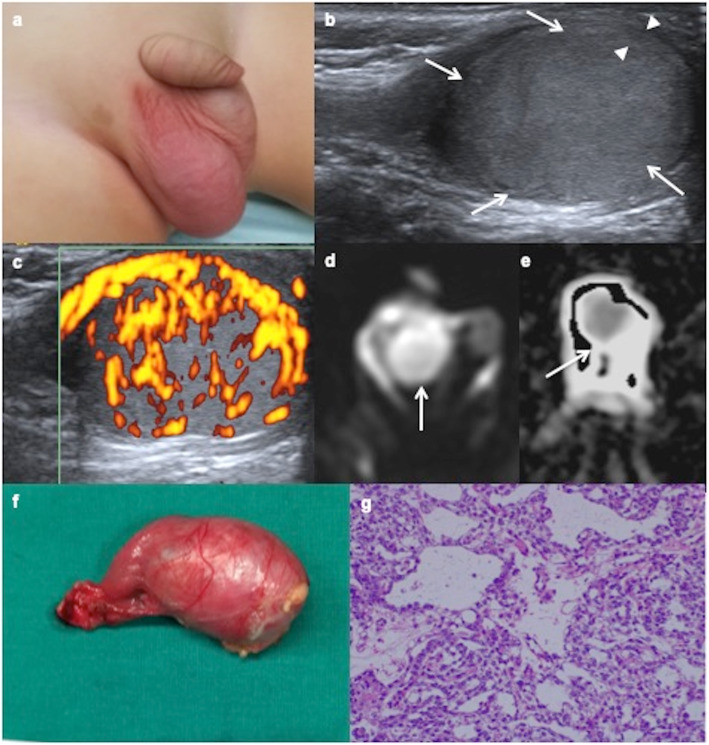
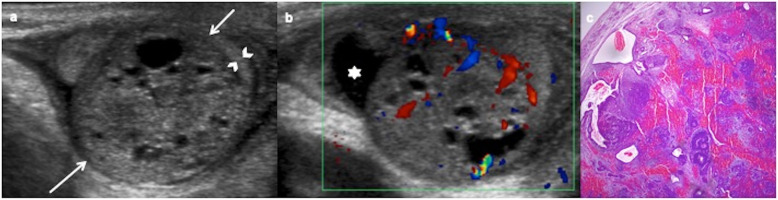
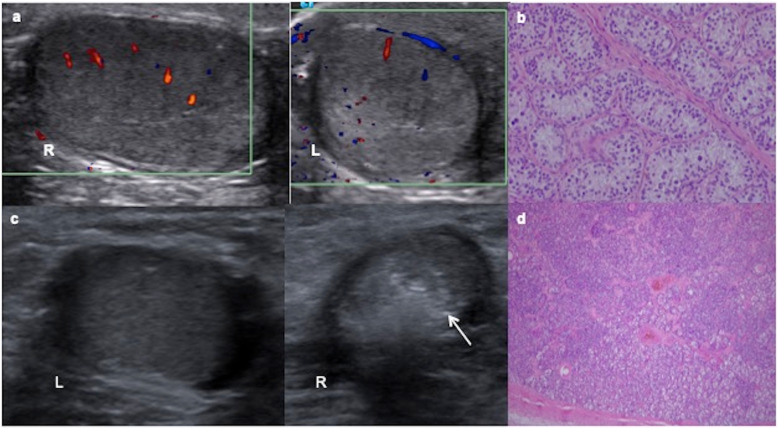
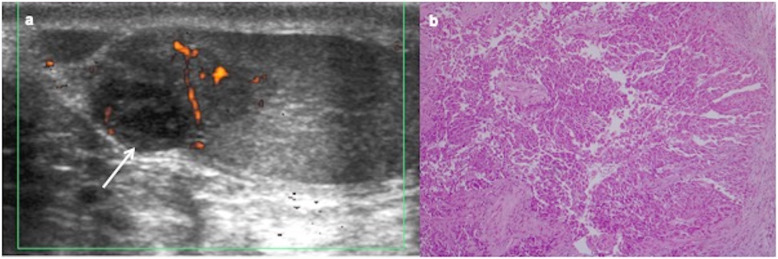
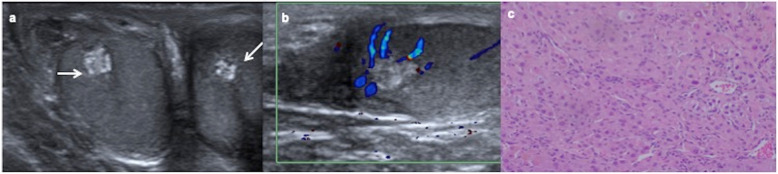
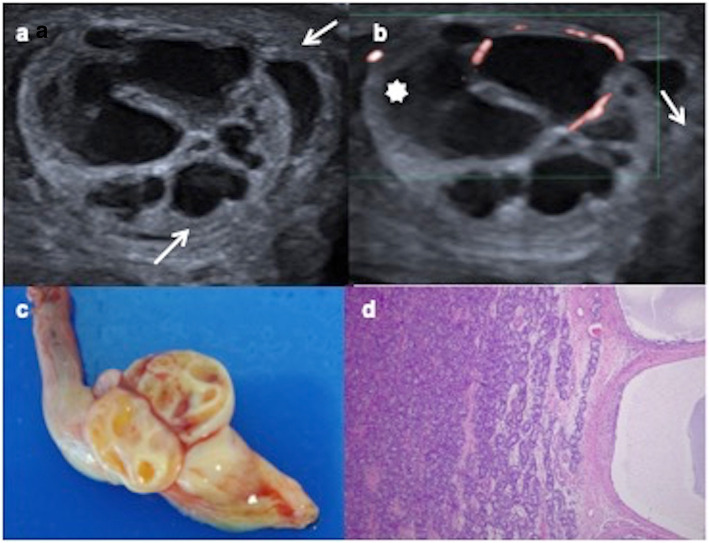
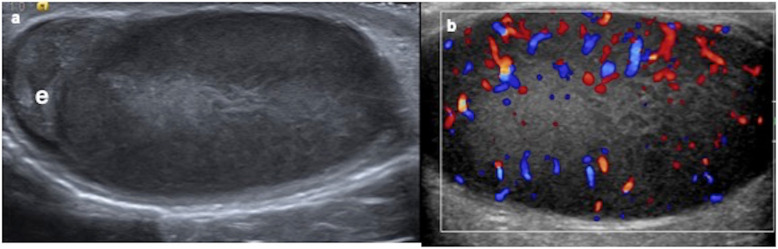
Testicular tumours are rare in children. Painless scrotal mass is the most frequent clinical presentation. Tumoural markers (alpha-fetoprotein, beta-human gonadotropin chorionic) and hormone levels (testosterone) contribute to the diagnosis and management of a testicular mass in boys. Ultrasonography is the best imaging modality to study testicular tumours. A benign tumour is suggested when ultrasonography shows a mainly cystic component, well-defined borders, echogenic rim or normal to increased echogenicity lesion when compared to the healthy testicular parenchyma. Malignant tumour is suspected when ultrasonography shows inhomogeneous, hypoechoic, not well-circumscribed or diffuse infiltration lesion. However, these ultrasonographic findings may overlap. Colour Doppler, power Doppler, elastography and contrast-enhanced ultrasonography are useful complementary methods to characterise the focal testicular lesions. Chest computerised tomography and abdominopelvic magnetic resonance are necessary to establish the extension in case of malignant proved tumours.Benign tumours are more frequent in prepuberal boys and malignant tumours in pubertal boys. Mature teratoma prepubertal-type is the most common histologic type. Testicular sparing surgery is the choice in benign tumours. Radical inguinal orchiectomy is indicated in malignant tumours. Prognostic is excellent.The purpose of our study is to show an approach to the diagnosis and management of the most frequent testicular tumours in children according to clinical manifestations, imaging findings and tumour markers levels based on histologically confirmed tumours in our hospital.
Keywords: Alpha-fetoprotein; Child; Testicular neoplasm; Ultrasonography, Doppler.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures







References
-
- Caballero Mora FJ, Muñoz Calvo MT, García Ros M, et al (2013) Testicular and paratesticular tumors during childhood and adolescence. An Pediatr (Barc) 78:6–13 - PubMed
-
- Poynter JN (2014) Epidemiology of Germ Cell Tumors. In: Frazier AL, Amatruda JF (eds) Pediatric germ cell tumors: biology treatment survivorship. Springer, Berlin Heidelberg p17-p36
Publication types
LinkOut - more resources
Full Text Sources
