

Major and ancillary features according to LI-RADS in the assessment of combined hepatocellular-cholangiocarcinoma
- PMID: 32463393
- PMCID: PMC7276649
- DOI: 10.2478/raon-2020-0029
Major and ancillary features according to LI-RADS in the assessment of combined hepatocellular-cholangiocarcinoma
Abstract
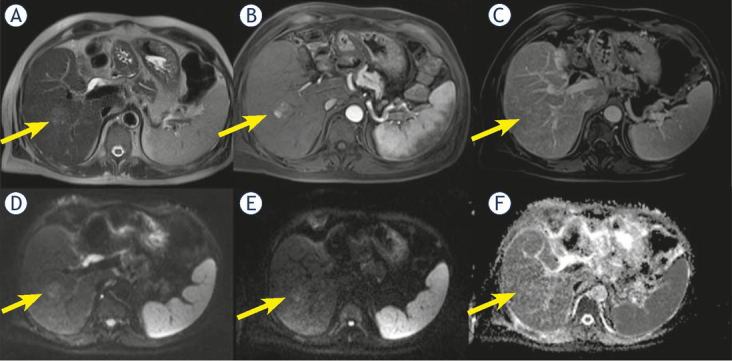
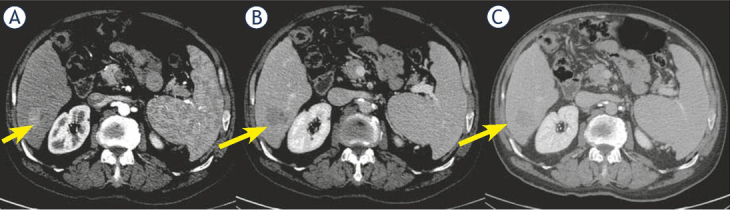
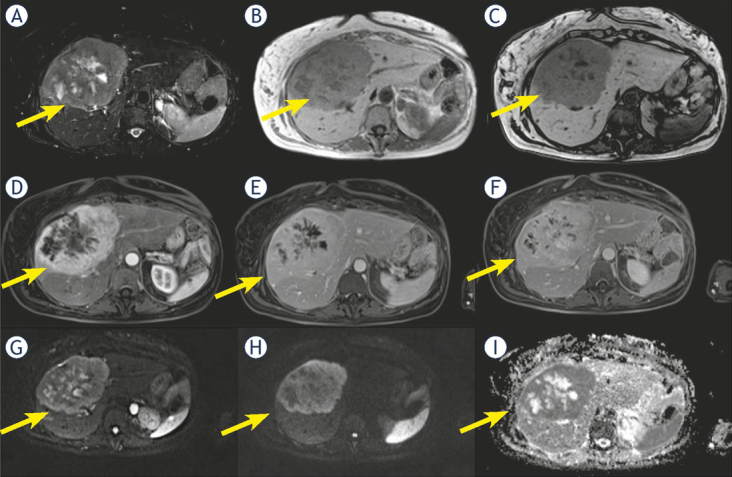
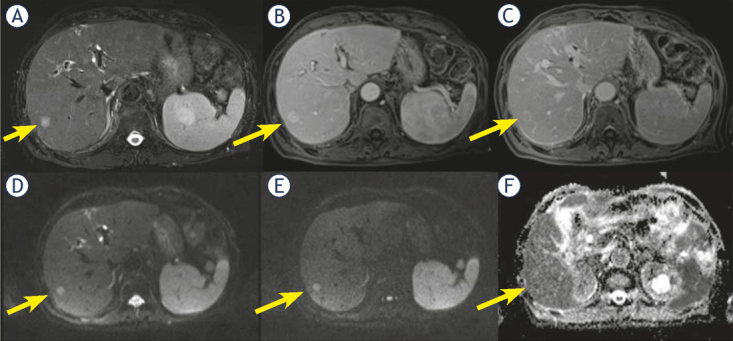
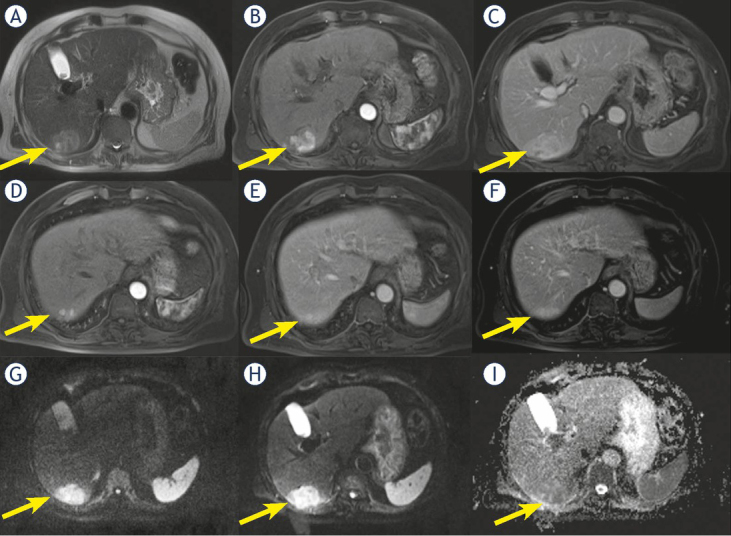
Background The aim of the study was to investigate the performance of the Liver Imaging Reporting and Data System (LI-RADS) v2018 for combined hepatocellular-cholangiocarcinoma (cHCC-CCA) identifying the features that allow an accurate characterization. Patients and methods Sixty-two patients (median age, 63 years; range, 38-80 years), with pre-surgical biopsy diagnosis of hepatocellular carcinoma (HCC) that underwent hepatic resection, comprised our retrospective study. All patients were subject to multidetector computed tomography (MDCT); 23 patients underwent to magnetic resonance (MR) study. The radiologist reported the presence of the HCC by using LIRADS v2018 assessing major and ancillary features. Results Final histological diagnosis was HCC for 51 patients and cHCC-CCA for 11 patients. The median nodule size was 46.0 mm (range 10-190 mm). For cHCC-CCA the median size was 33.5 mm (range 20-80 mm), for true HCC the median size was 47.5 mm (range 10-190 mm). According to LIRADS categories: 54 (87.1%) nodules as defined as LR-5, 1 (1.6%) as LR-3, and 7 (11.3%) as LR-M. Thirty-nine nodules (63%) showed hyper-enhancement in arterial phase; among them 4 were cHCC-CCA (36.4% of cHCC-CCA) and 35 (68.6%) true HCC. Forty-three nodules (69.3%) showed washout appearance; 6 cHCC-CCAs (54.5% of cHCC-CCA) and 37 true HCC (72.5%) had this feature. Only two cHCC-CCA patients (18.2% of cHCC-CCA) showed capsule appearance. Five cHCC-CCA (71.4% of cHCC-CCA) showed hyperintensity on T2-W sequences while two (28.6%) showed inhomogeneous signal in T2-W. All cHCC-CCA showed restricted diffusion. Seven cHCC-CCA patients showed a progressive contrast enhancement and satellite nodules. Conclusions The presence of satellite nodules, hyperintense signal on T2-W, restricted diffusion, the absence of capsule appearance in nodule that shows peripheral and progressive contrast enhancement are suggestive features of cHCC-CCA.
Keywords: combined hepatocellular-cholangiocarcinoma; hepatocellular carcinoma; magnetic resonance imaging; multidetector computed tomography.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical