

Community-level interventions for pre-eclampsia (CLIP) in Mozambique: A cluster randomised controlled trial
- PMID: 32464527
- PMCID: PMC7471842
- DOI: 10.1016/j.preghy.2020.05.006
Community-level interventions for pre-eclampsia (CLIP) in Mozambique: A cluster randomised controlled trial
Abstract
Objectives: Pregnancy hypertension is the third leading cause of maternal mortality in Mozambique and contributes significantly to fetal and neonatal mortality. The objective of this trial was to assess whether task-sharing care might reduce adverse pregnancy outcomes related to delays in triage, transport, and treatment.
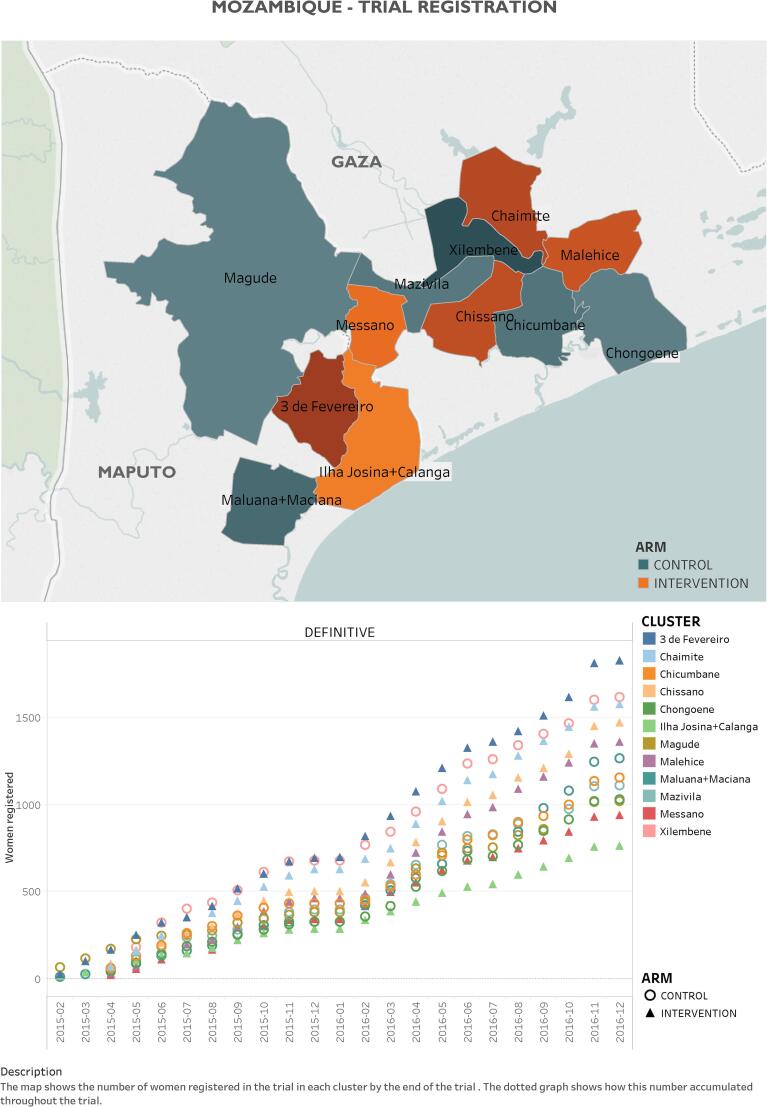
Study design: The Mozambique Community-Level Interventions for Pre-eclampsia (CLIP) cluster randomised controlled trial (NCT01911494) recruited pregnant women in 12 administrative posts (clusters) in Maputo and Gaza Provinces. The CLIP intervention (6 clusters) consisted of community engagement, community health worker-provided mobile health-guided clinical assessment, initial treatment, and referral to facility either urgently (<4hrs) or non-urgently (<24hrs), dependent on algorithm-defined risk. Treatment effect was estimated by multi-level logistic regression modelling, adjusted for prognostically-significant baseline variables. Predefined secondary analyses included safety and evaluation of the intensity of CLIP contacts.
Main outcome measures: 20% reduction in composite of maternal, fetal, and newborn mortality and major morbidity.
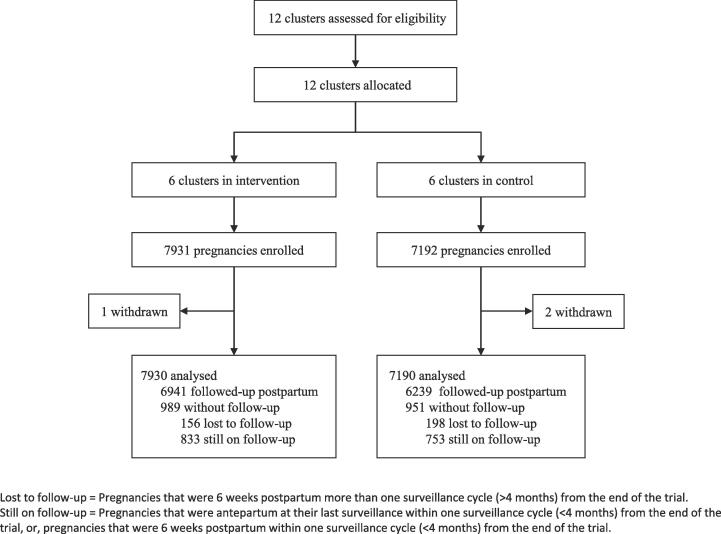
Results: 15,013 women (15,123 pregnancies) were recruited in intervention (N = 7930; 2·0% loss to follow-up (LTFU)) and control (N = 7190; 2·8% LTFU) clusters. The primary outcome did not differ between intervention and control clusters (adjusted odds ratio (aOR) 1·31, 95% confidence interval (CI) [0·70, 2·48]; p = 0·40). Compared with intervention arm women without CLIP contacts, those with ≥8 contacts experienced fewer primary outcomes (aOR 0·79 (95% CI 0·63, 0·99); p = 0·041), primarily due to improved maternal outcomes (aOR 0·72 (95% CI 0·53, 0·97); p = 0·033).
Interpretation: As generally implemented, the CLIP intervention did not improve pregnancy outcomes; community implementation of the WHO eight contact model may be beneficial.
Funding: The University of British Columbia (PRE-EMPT), a grantee of the Bill & Melinda Gates Foundation (OPP1017337).
Keywords: Cluster randomized controlled trial; Community engagement; Community health worker; Mobile health; Mozambique; Pregnancy hypertension.
Copyright © 2020 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
We declare no competing interests. BAP, LAM and PvD acknowledge that the intellectual property related to the miniPIERS prediction model used in the CLIP trials was transferred in its entirety from the University of British Columbia to them, among other inventors, prior to the trial. They have no financial benefit from the use of the model based on the transfer.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
