

Preliminary CT findings of coronavirus disease 2019 (COVID-19)
- PMID: 32464579
- PMCID: PMC7214302
- DOI: 10.1016/j.clinimag.2020.04.042
Preliminary CT findings of coronavirus disease 2019 (COVID-19)
Abstract
Objectives: Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). This paper aims to examine the CT imaging characteristics of COVID-19.
Methods: We evaluated CT images obtained between 10 January 2019 and 16 February 2020 at Taihe Hospital. Scans were conducted 2-6 times per patient and the re-testing interval was 2-7 days. Ninety-five patients with positive SARS-CoV-2 nucleic acid test results were included in this study and we retrospectively analysed their CT imaging characteristics.
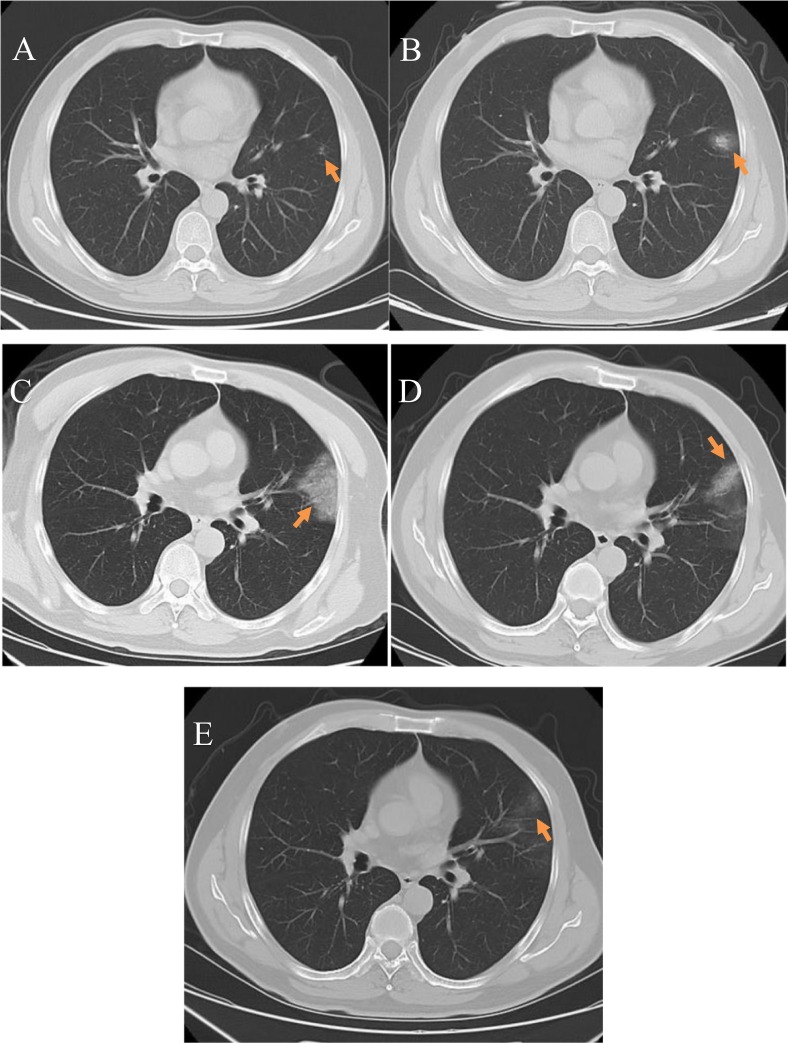
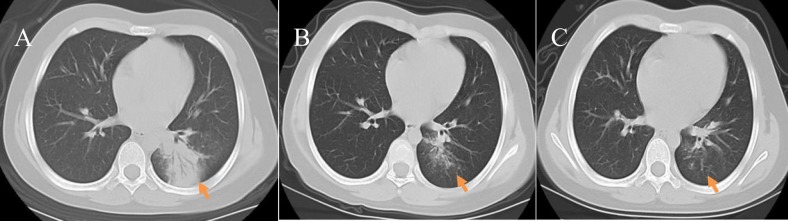
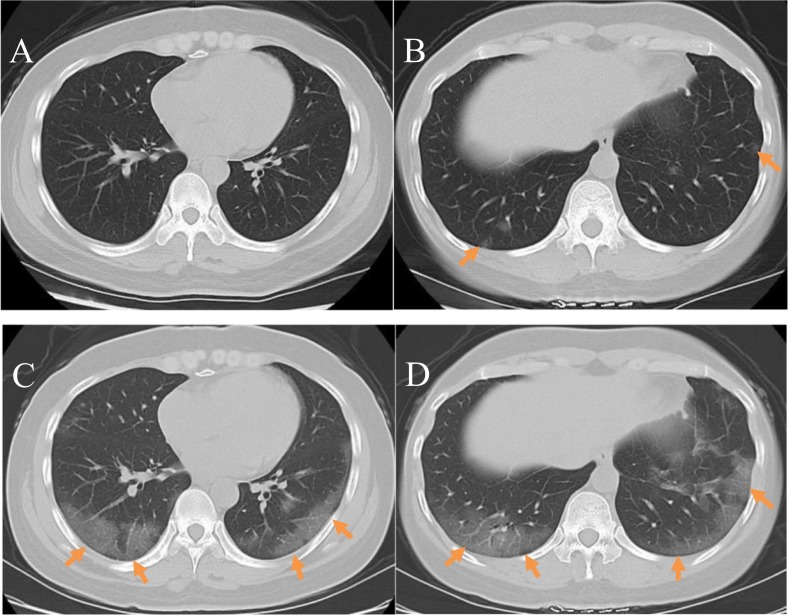
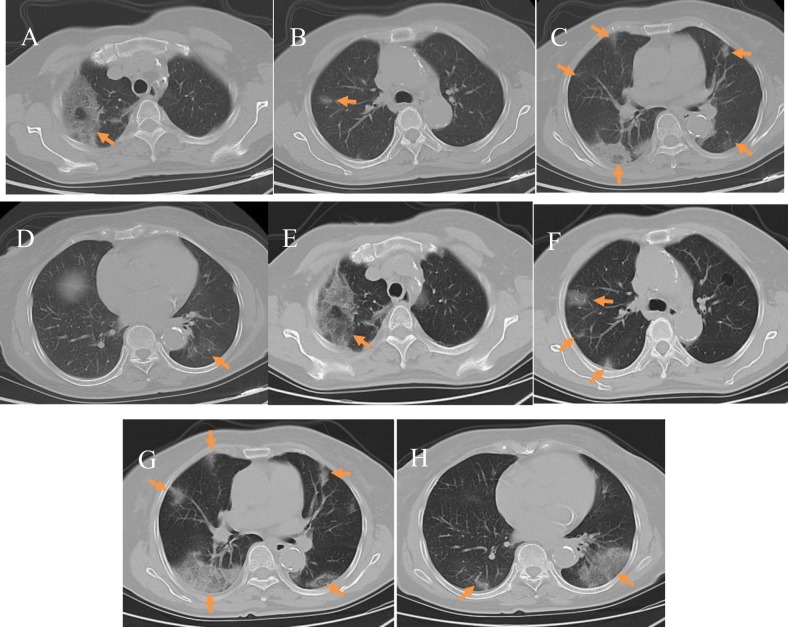
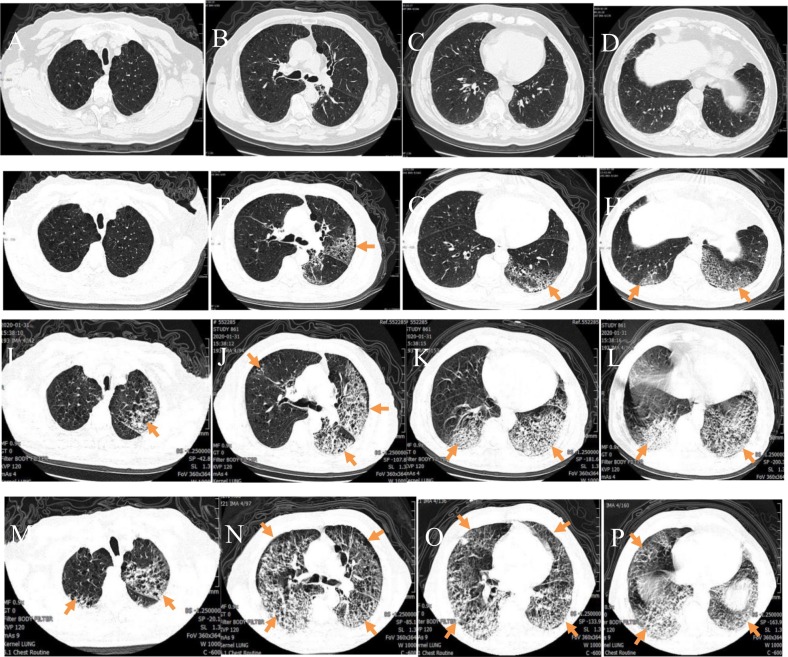
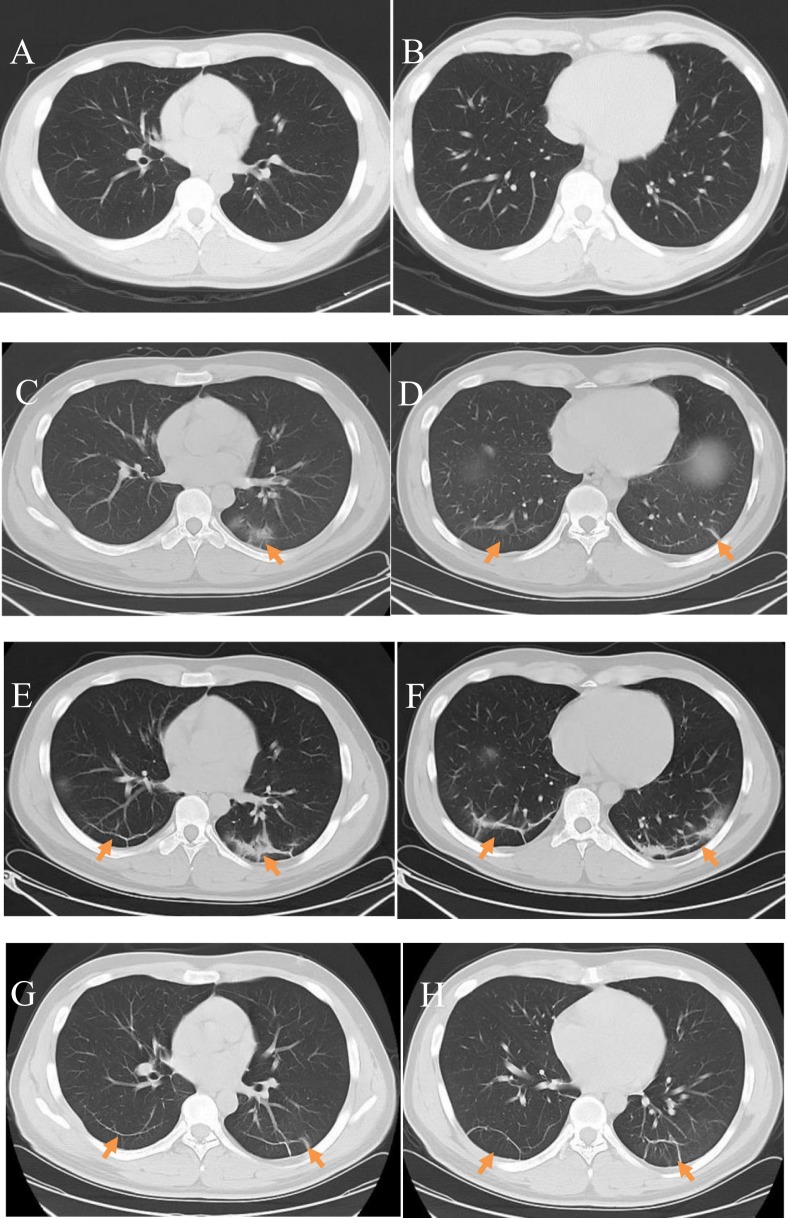
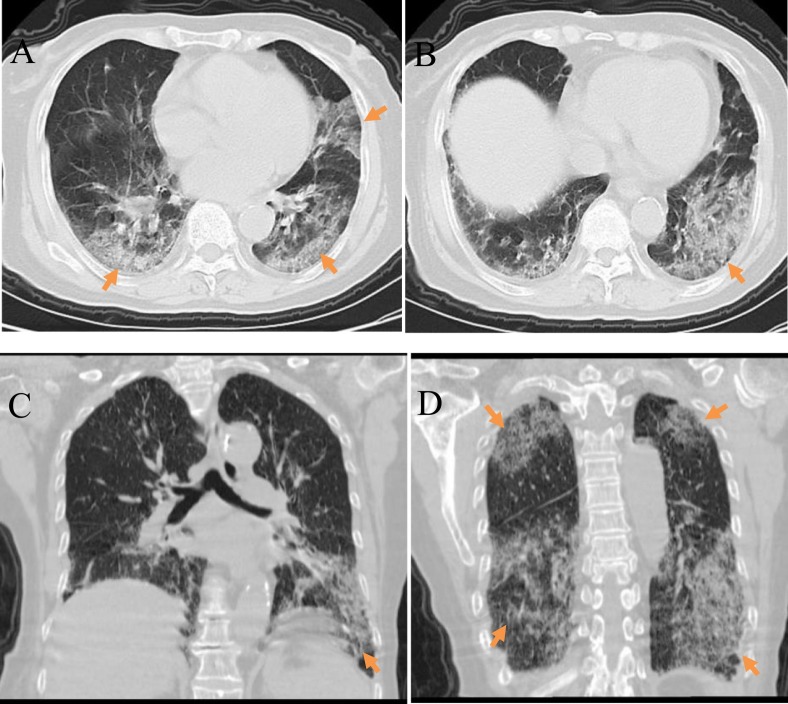
Results: Ninety-five patients underwent 2-3 SARS-CoV-2 nucleic acid tests and received a definitive diagnosis of COVID-19. Fifty-three were male and 42 were female, and their mean age was 42 ± 12 years (range: 10 months to 81 years). Sixty-nine patients (72.6%) experienced fever, fatigue, and dry cough, while 15 (15.8%) had poor appetite and fatigue, and 11 (11.6%) had a dry cough and no fever. On CT imaging, early stage patients (n = 53, 55.8%) showed peripheral subpleural ground-glass opacities; these were mainly local patches (22/53, 41.5%), while some lesions were accompanied by interlobular septal thickening. Thirty-four (35.8%) patients were classified in the 'progression stage' based on CT imaging; these patients typically showed lesions in multiple lung segments and lobes (21/34,61.8%), and an uneven increase in ground-glass opacity density accompanied by consolidation and grid-like or cord-like shadows(30.5%). Two patients (2.1%) showed a severe presentation on CT. These showed diffuse bilateral lung lesions, mixed ground-glass opacities and consolidation with cord-like interstitial thickening and air bronchograms, entire lung involvement with a "white lung" presentation, and mild pleural effusion. Six patients in remission (6.3%), visible lesion absorption, fibrotic lesions. Based on clinical signs, 71 (74.7%), 22 (23.2%), and 2 (2.1%) patients had mild or moderate, severe, and critical disease, respectively. Within the follow-up period, 93 patients recovered and were discharged, including the 53 early stage patients and 34 progression stage patients. The length of hospitalisation was 7-28 days (mean: 10 ± 3.5 days). On discharge, lesions were significantly reduced in area and had in many cases completely disappeared, while slight pulmonary fibrosis was present in some patients. One severe stage patient was still hospitalised at the end of the follow-up period and the other severe stage patient died. The overall mortality rate was 1.05%.
Conclusions: Understanding the CT imaging characteristics of COVID-19 is important for early lesion detection, determining the nature of lesions, and assessing disease severity.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
References
-
- National Health Commission, State Administration of Traditional Chinese Medicine Coronavirus disease 2019 diagnosis and treatment protocol (interim 7th edition) [EB/OL] http://www.nhc.gov.cn/yzygj/s7653p/202002/8334a8326dd94d329df351d7da8aef...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
