

Ethnic and socioeconomic differences in SARS-CoV-2 infection: prospective cohort study using UK Biobank
- PMID: 32466757
- PMCID: PMC7255908
- DOI: 10.1186/s12916-020-01640-8
Ethnic and socioeconomic differences in SARS-CoV-2 infection: prospective cohort study using UK Biobank
Abstract
Background: Understanding of the role of ethnicity and socioeconomic position in the risk of developing SARS-CoV-2 infection is limited. We investigated this in the UK Biobank study.
Methods: The UK Biobank study recruited 40-70-year-olds in 2006-2010 from the general population, collecting information about self-defined ethnicity and socioeconomic variables (including area-level socioeconomic deprivation and educational attainment). SARS-CoV-2 test results from Public Health England were linked to baseline UK Biobank data. Poisson regression with robust standard errors was used to assess risk ratios (RRs) between the exposures and dichotomous variables for being tested, having a positive test and testing positive in hospital. We also investigated whether ethnicity and socioeconomic position were associated with having a positive test amongst those tested. We adjusted for covariates including age, sex, social variables (including healthcare work and household size), behavioural risk factors and baseline health.
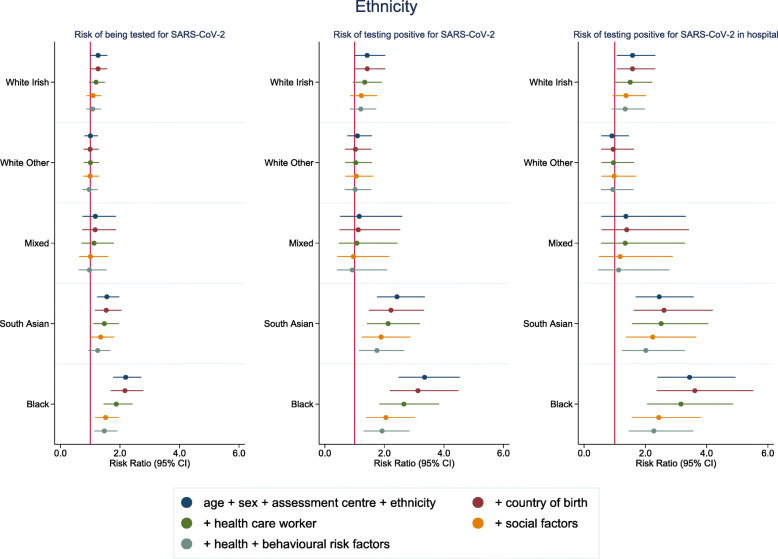
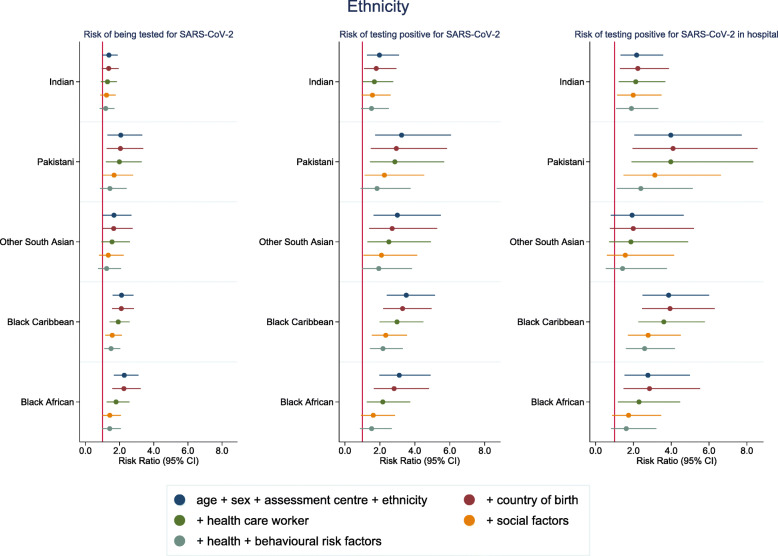
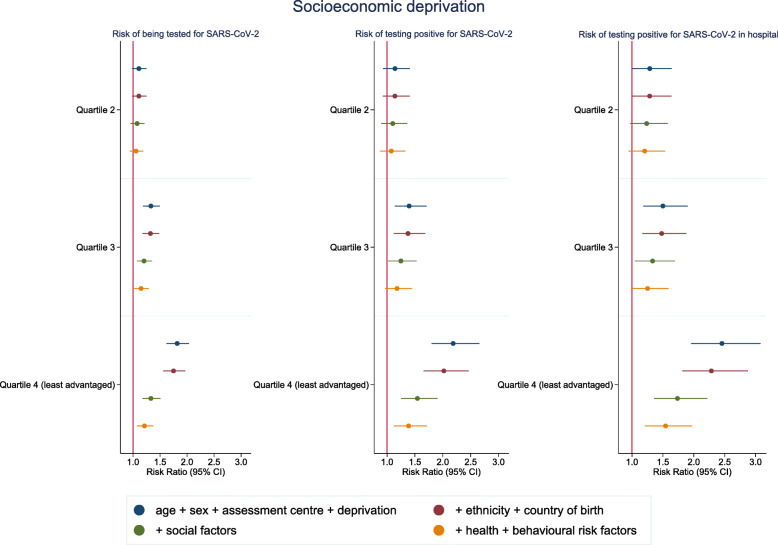
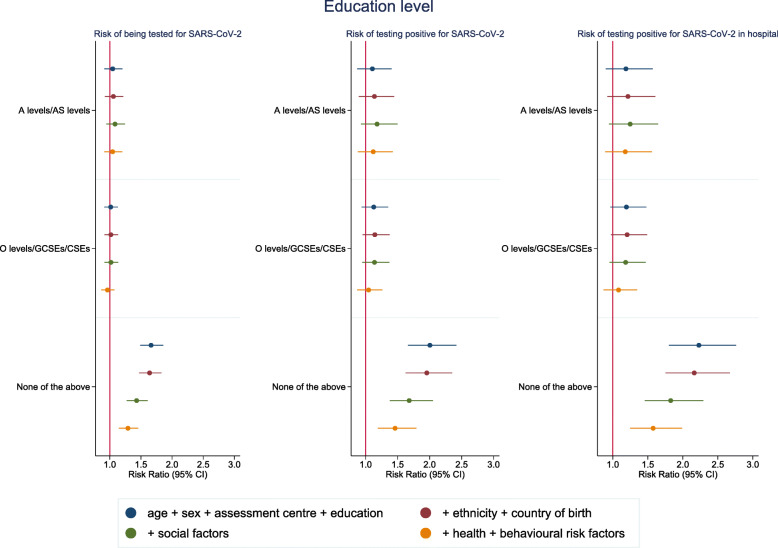
Results: Amongst 392,116 participants in England, 2658 had been tested for SARS-CoV-2 and 948 tested positive (726 in hospital) between 16 March and 3 May 2020. Black and south Asian groups were more likely to test positive (RR 3.35 (95% CI 2.48-4.53) and RR 2.42 (95% CI 1.75-3.36) respectively), with Pakistani ethnicity at highest risk within the south Asian group (RR 3.24 (95% CI 1.73-6.07)). These ethnic groups were more likely to be hospital cases compared to the white British. Adjustment for baseline health and behavioural risk factors led to little change, with only modest attenuation when accounting for socioeconomic variables. Socioeconomic deprivation and having no qualifications were consistently associated with a higher risk of confirmed infection (RR 2.19 for most deprived quartile vs least (95% CI 1.80-2.66) and RR 2.00 for no qualifications vs degree (95% CI 1.66-2.42)).
Conclusions: Some minority ethnic groups have a higher risk of confirmed SARS-CoV-2 infection in the UK Biobank study, which was not accounted for by differences in socioeconomic conditions, baseline self-reported health or behavioural risk factors. An urgent response to addressing these elevated risks is required.
Keywords: COVID-19; Coronavirus; Ethnicity; Health inequality; Inequality; Infectious disease; Pandemic; SARS-CoV-2; Social factors.
Conflict of interest statement
JPP is a member of the UK Biobank Steering Committee. Apart from the funding acknowledged below, we declare no other competing interests.
Figures
Comment in
-
Ethnicity and COVID-19 infection: are the pieces of the puzzle falling into place?BMC Med. 2020 Jul 1;18(1):206. doi: 10.1186/s12916-020-01669-9. BMC Med. 2020. PMID: 32605617 Free PMC article. No abstract available.
References
-
- World Health Organization: Coronavirus disease 2019 (COVID-19): situation report – 91. In. Geneva: World Health Organization; 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio.... Accessed 20 Apr 2020.
-
- Sattar N, McInnes IB, JJV M: Obesity a risk factor for severe COVID-19 infection: multiple potential mechanisms. Circulation 2020. In press. 10.1161/CIRCULATIONAHA.120.047659. - PubMed
-
- Myers EM. Compounding Health Risks and Increased Vulnerability to SARS-CoV-2 for Racial and Ethnic Minorities and Low Socioeconomic Status Individuals in the United States. Preprints. 2020;2020040234. 10.20944/preprints202004.0234.v1.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
