

A multi-center analysis of single-fraction versus hypofractionated stereotactic radiosurgery for the treatment of brain metastasis
- PMID: 32466775
- PMCID: PMC7257186
- DOI: 10.1186/s13014-020-01522-6
A multi-center analysis of single-fraction versus hypofractionated stereotactic radiosurgery for the treatment of brain metastasis
Abstract
Background: Hypofractionated-SRS (HF-SRS) may allow for improved local control and a reduced risk of radiation necrosis compared to single-fraction-SRS (SF-SRS). However, data comparing these two treatment approaches are limited. The purpose of this study was to compare clinical outcomes between SF-SRS versus HF-SRS across our multi-center academic network.
Methods: Patients treated with SF-SRS or HF-SRS for brain metastasis from 2013 to 2018 across 5 radiation oncology centers were retrospectively reviewed. SF-SRS dosing was standardized, whereas HF-SRS dosing regimens were variable. The co-primary endpoints of local control and radiation necrosis were estimated using the Kaplan Meier method. Multivariate analysis using Cox proportional hazards modeling was performed to evaluate the impact of select independent variables on the outcomes of interest. Propensity score adjustments were used to reduce the effects confounding variables. To assess dose response for HF-SRS, Biologic Effective Dose (BED) assuming an α/β of 10 (BED10) was used as a surrogate for total dose.
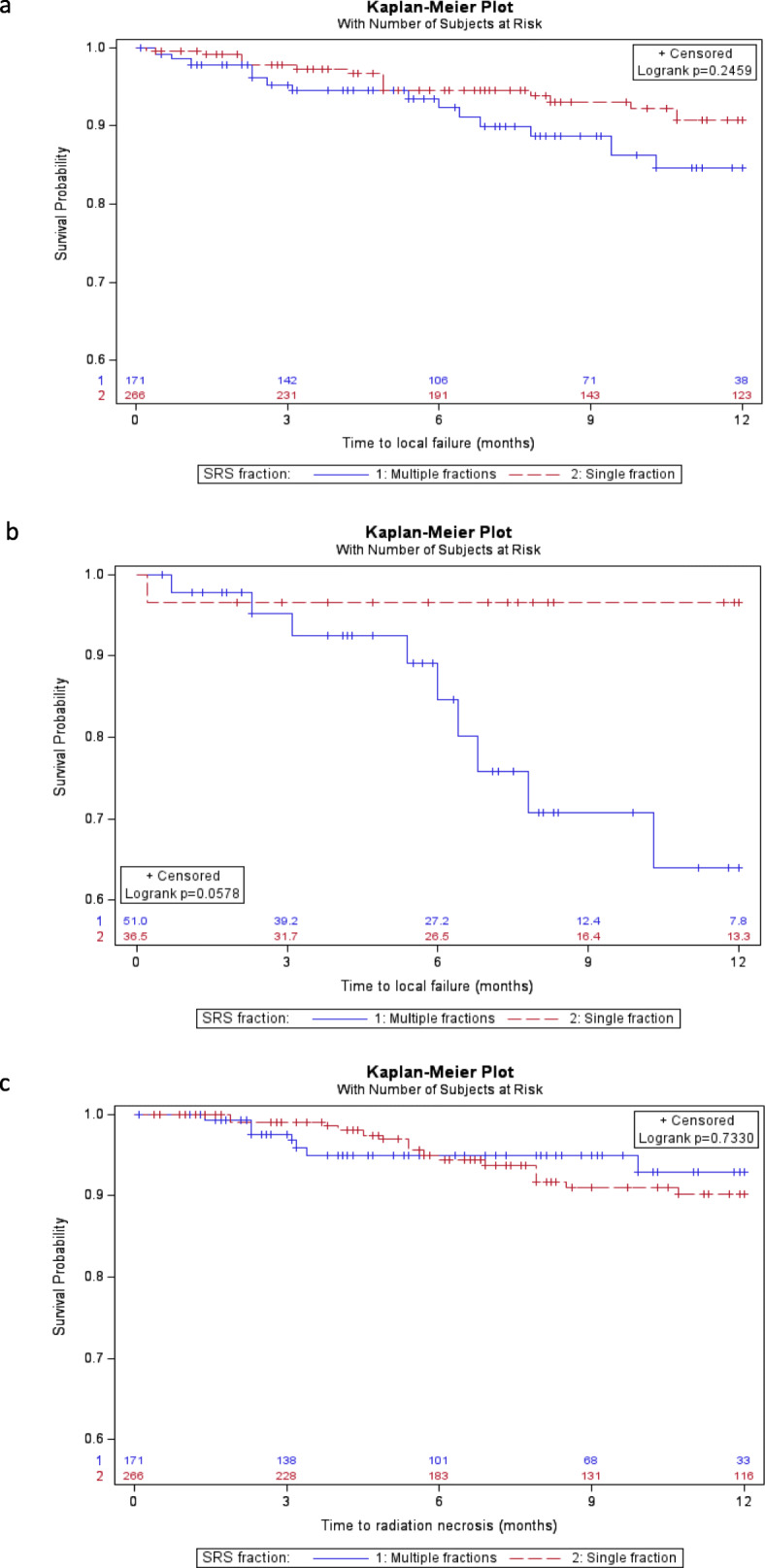
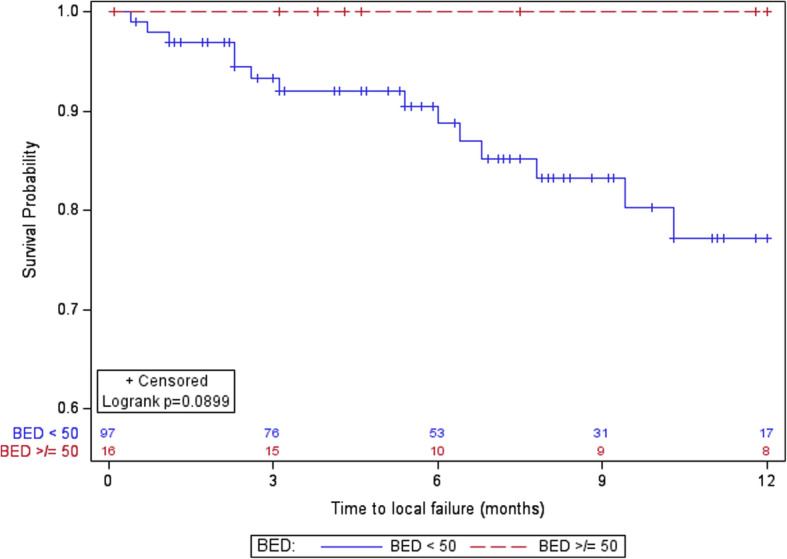
Results: One-hundred and fifty six patients with 335 brain metastasis treated with SF-SRS (n = 222 lesions) or HF-SRS (n = 113 lesions) were included. Prior whole brain radiation was given in 33% (n = 74) and 34% (n = 38) of lesions treated with SF-SRS and HF-SRS, respectively (p = 0.30). After a median follow up time of 12 months in each cohort, the adjusted 1-year rate of local control and incidence of radiation necrosis was 91% (95% CI 86-96%) and 85% (95% CI 75-95%) (p = 0.26) and 10% (95% CI 5-15%) and 7% (95% CI 0.1-14%) (p = 0.73) for SF-SRS and HF-SRS, respectively. For lesions > 2 cm, the adjusted 1 year local control was 97% (95% CI 84-100%) for SF-SRS and 64% (95% CI 43-85%) for HF-SRS (p = 0.06). On multivariate analysis, SRS fractionation was not associated with local control and only size ≤2 cm was associated with a decreased risk of developing radiation necrosis (HR 0.21; 95% CI 0.07-0.58, p < 0.01). For HF-SRS, 1 year local control was 100% for lesions treated with a BED10 ≥ 50 compared to 77% (95% CI 65-88%) for lesions that received a BED10 < 50 (p = 0.09).
Conclusions: In this comparison study of dose fractionation for the treatment of brain metastases, there was no difference in local control or radiation necrosis between HF-SRS and SF-SRS. For HF-SRS, a BED10 ≥ 50 may improve local control.
Keywords: Biologic effective dose; Brain metastasis; GammaKnife; Hypofractionated stereotactic radiosurgery; Normal tissue injury; Stereotactic radiosurgery.
Conflict of interest statement
Dr. Mishra reports receiving personal fees from Varian, outside of the scope of the current manuscript.
Figures
Similar articles
-
Hypofractionated versus single-fraction stereotactic radiosurgery for the treatment of brain metastases: A systematic review and meta-analysis.Clin Neurol Neurosurg. 2021 Jul;206:106645. doi: 10.1016/j.clineuro.2021.106645. Epub 2021 Apr 20. Clin Neurol Neurosurg. 2021. PMID: 33984752
-
Repeat stereotactic radiosurgery as salvage therapy for locally recurrent brain metastases previously treated with radiosurgery.J Neurosurg. 2017 Jul;127(1):148-156. doi: 10.3171/2016.5.JNS153051. Epub 2016 Aug 5. J Neurosurg. 2017. PMID: 27494815
-
Single-fraction radiosurgery versus fractionated stereotactic radiotherapy in patients with brain metastases: a comparative study.Clin Exp Metastasis. 2020 Jun;37(3):425-434. doi: 10.1007/s10585-020-10031-5. Epub 2020 Mar 17. Clin Exp Metastasis. 2020. PMID: 32185576
-
Single-Fraction Versus Multifraction (3 × 9 Gy) Stereotactic Radiosurgery for Large (>2 cm) Brain Metastases: A Comparative Analysis of Local Control and Risk of Radiation-Induced Brain Necrosis.Int J Radiat Oncol Biol Phys. 2016 Jul 15;95(4):1142-8. doi: 10.1016/j.ijrobp.2016.03.013. Epub 2016 Mar 19. Int J Radiat Oncol Biol Phys. 2016. PMID: 27209508
-
Single- and hypofractionated stereotactic radiosurgery for large (> 2 cm) brain metastases: a systematic review.J Neurooncol. 2021 Aug;154(1):25-34. doi: 10.1007/s11060-021-03805-8. Epub 2021 Jul 15. J Neurooncol. 2021. PMID: 34268640
Cited by
-
Breast cancer subtype predicts clinical outcomes after stereotactic radiation for brain metastases.J Neurooncol. 2021 May;152(3):591-601. doi: 10.1007/s11060-021-03735-5. Epub 2021 Mar 19. J Neurooncol. 2021. PMID: 33742358
-
Association of increasing gross tumor volume dose with tumor volume reduction and local control in fractionated stereotactic radiosurgery for unresected brain metastases.Radiat Oncol. 2024 Jul 27;19(1):95. doi: 10.1186/s13014-024-02487-6. Radiat Oncol. 2024. PMID: 39061079 Free PMC article.
-
Outcomes in Patients with Intact and Resected Brain Metastasis Treated with 5-Fraction Stereotactic Radiosurgery.Adv Radiat Oncol. 2022 Dec 29;8(2):101166. doi: 10.1016/j.adro.2022.101166. eCollection 2023 Mar-Apr. Adv Radiat Oncol. 2022. PMID: 36845614 Free PMC article.
-
The dosimetric parameters impact on local recurrence in stereotactic radiotherapy for brain metastases.Br J Radiol. 2024 Mar 28;97(1156):820-827. doi: 10.1093/bjr/tqae029. Br J Radiol. 2024. PMID: 38377402 Free PMC article.
-
Efficacy of Radiotherapy for Oligometastatic Lung Cancer and Irradiation Methods Based on Metastatic Site.Cancers (Basel). 2025 Aug 4;17(15):2569. doi: 10.3390/cancers17152569. Cancers (Basel). 2025. PMID: 40805265 Free PMC article. Review.
References
-
- Patchell RA, Tibbs PA, Regine WF, Dempsey RJ, Mohiuddin M, Kryscio RJ, et al. Postoperative radiotherapy in the treatment of single metastases to the brain: a randomized trial. J Am Med Assoc. 1998;280:1485–1489. - PubMed
-
- Shaw E, Scott C, Souhami L, Dinapoli R, Kline R, Loeffler J, et al. Single dose radiosurgical treatment of recurrent previously irradiated primary brain tumors and brain metastases: Final report of RTOG protocol 90–05. Int J Radiat Oncol Biol Phys. 2000;47:291–298. - PubMed
-
- Chang EL, Wefel JS, Hess KR, Allen PK, Lang FF, Kornguth DG, et al. Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: a randomised controlled trial. Lancet Oncol. 2009;10:1037–1044. - PubMed
-
- Aoyama H, Shirato H, Tago M, Nakagawa K, Toyoda T, Hatano K, et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: a randomized controlled trial. J Am Med Assoc. 2006;295:2483–2491. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
