

National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study
- PMID: 32467098
- PMCID: PMC7254147
- DOI: 10.1136/bmj.m1590
National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study
Abstract
Objective: To systematically review and provide information on the incidence of psoriasis and quantify global, regional, and country specific estimates of its prevalence.
Design: Systematic review and meta-analysis.
Data sources: Medline, Embase, Web of Science, SciELO, Korean Journal Databases, Russian Science Citation Index, WPRIM, SaudiMedLit, Informit, IndMed, and HERDIN were searched systematically from their inception dates to October 2019.
Methods: Studies were included if they reported on the incidence or prevalence of psoriasis in the general population. Incidence data were summarised descriptively, whereas bayesian hierarchical models were fitted to estimate the global, regional, and country specific prevalence of psoriasis.
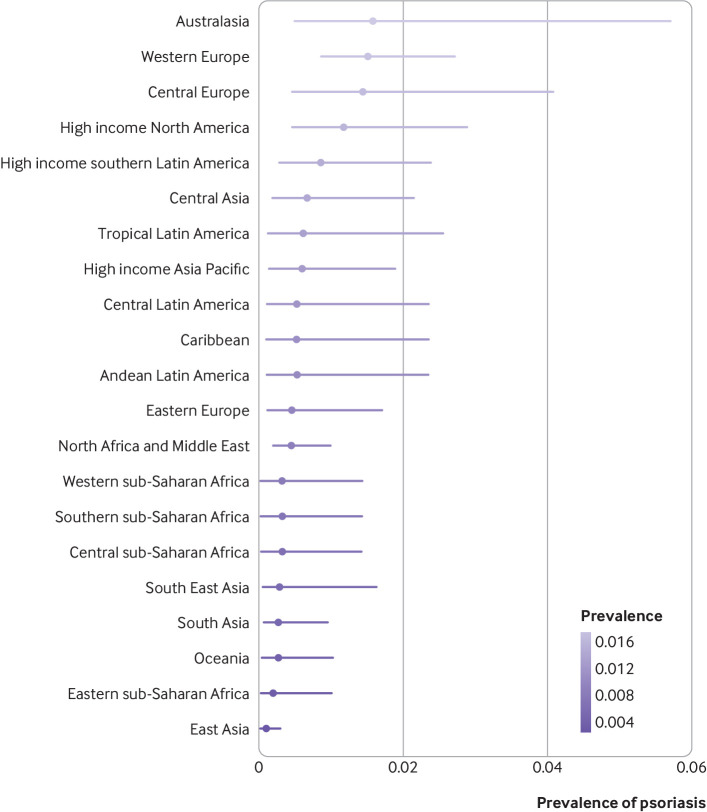
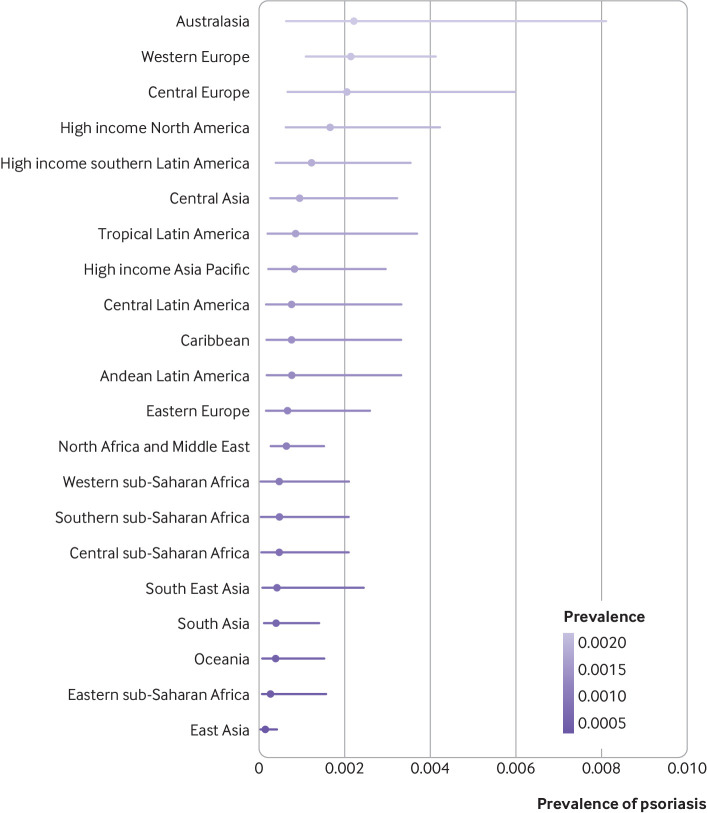
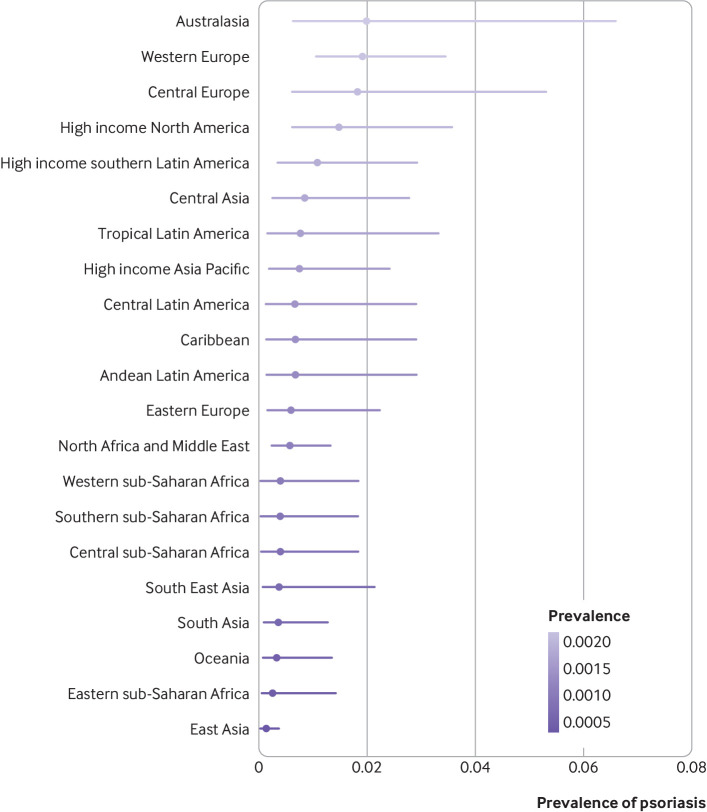
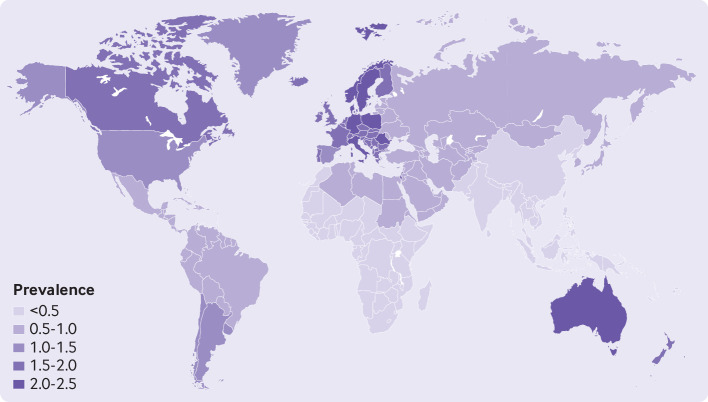
Results: 41 164 records were identified and 168 studies met the inclusion criteria. In adults, the incidence of psoriasis varied from 30.3 per 100 000 person years (95% confidence interval 26.6 to 34.1) in Taiwan to 321.0 per 100 000 person years in Italy. The prevalence of psoriasis varied from 0.14% (95% uncertainty interval 0.05% to 0.40%) in east Asia to 1.99% (0.64% to 6.60%) in Australasia. The prevalence of psoriasis was also high in western Europe (1.92%, 1.07% to 3.46%), central Europe (1.83%, 0.62% to 5.32%), North America (1.50%, 0.63% to 3.60%), and high income southern Latin America (1.10%, 0.36% to 2.96%).
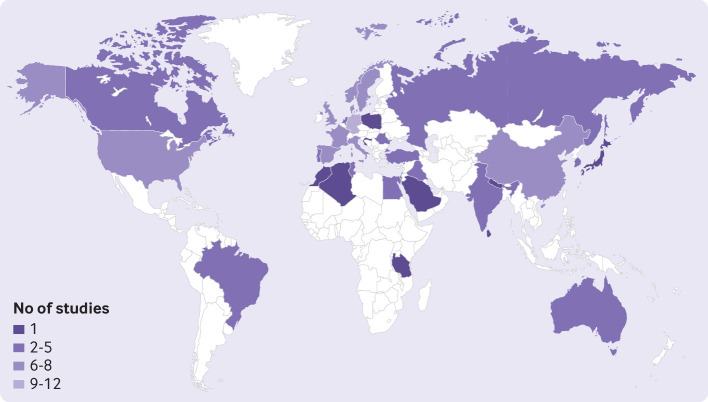
Conclusions: Eighty one per cent of the countries of the world lack information on the epidemiology of psoriasis. The disease occurs more frequently in adults than in children. Psoriasis is unequally distributed across geographical regions; it is more frequent in high income countries and in regions with older populations. The estimates provided can help guide countries and the international community when making public health decisions on the appropriate management of psoriasis and assessing its natural history over time.
Systematic review registration: PROSPERO CRD42019160817.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from the Leo Foundation, Abbvie, Eli Lilly UK and Company Ltd, Novartis Pharma AG, UCB, and Almirall for the submitted work; CEMG reports receiving honorariums or research grants from AbbVie, Almirall, Celgene, Eli Lilly, Galderma, Janssen, LEO Pharma, Novartis, Pfizer, Sandoz, Sanofi, and UCB Pharma; DMA reports research grants from AbbVie, Almirall, Celgene, Eli Lilly, Novartis, UCB, and the Leo Foundation; MA reports receiving speakers honorariums or grants from, or participated in clinical trials or health services research projects for Abbott/AbbVie, Almirall, Amgen, Biogen Idec, Boehringer Ingelheim, Celgene, Centocor, Eli Lilly, Forward Pharma, Galderma, GSK, Hexal, Janssen, LEO Pharma, Medac, MSD, Novartis, Pfizer, Sandoz, Teva, TK, Trevi, and Xenoport; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous