

Brain Imaging Use and Findings in COVID-19: A Single Academic Center Experience in the Epicenter of Disease in the United States
- PMID: 32467191
- PMCID: PMC7357666
- DOI: 10.3174/ajnr.A6610
Brain Imaging Use and Findings in COVID-19: A Single Academic Center Experience in the Epicenter of Disease in the United States
Abstract
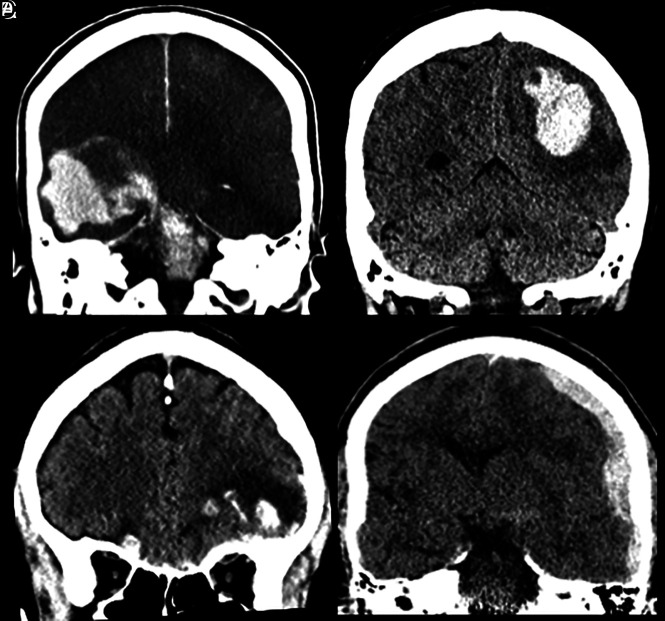
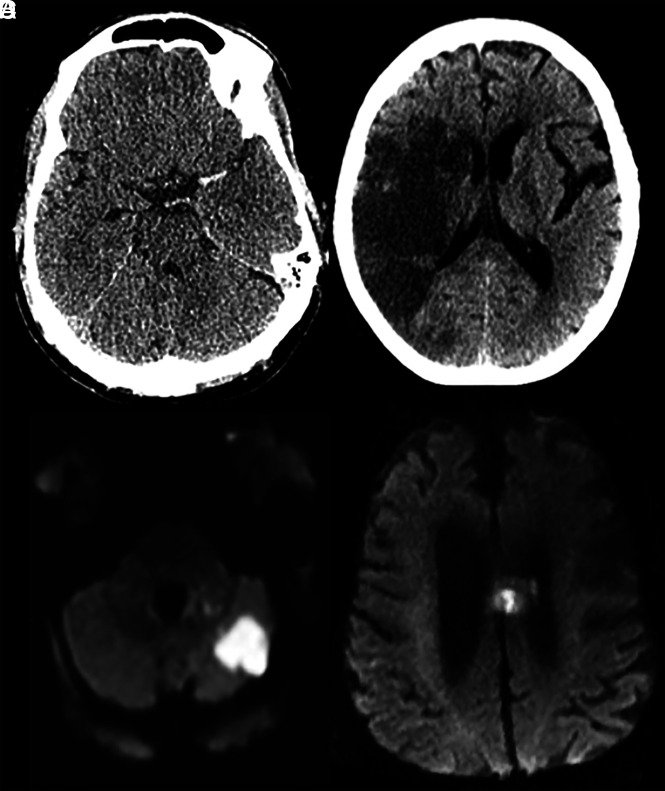
Coronavirus disease 2019 (COVID-19) is a serious public health crisis and can have neurologic manifestations. This is a retrospective observational case series performed March 1-31, 2020, at New York University Langone Medical Center campuses. Clinical and imaging data were extracted, reviewed, and analyzed. Two hundred forty-two patients with COVID-19 underwent CT or MRI of the brain within 2 weeks after the positive result of viral testing (mean age, 68.7 ± 16.5 years; 150 men/92 women [62.0%/38.0%]). The 3 most common indications for imaging were altered mental status (42.1%), syncope/fall (32.6%), and focal neurologic deficit (12.4%). The most common imaging findings were nonspecific white matter microangiopathy (134/55.4%), chronic infarct (47/19.4%), acute or subacute ischemic infarct (13/5.4%), and acute hemorrhage (11/4.5%). No patients imaged for altered mental status demonstrated acute ischemic infarct or acute hemorrhage. White matter microangiopathy was associated with higher 2-week mortality (P < .001). Our data suggest that in the absence of a focal neurologic deficit, brain imaging in patients with early COVID-19 with altered mental status may not be revealing.
© 2020 by American Journal of Neuroradiology.
Figures
References
-
- COVID-19 United States Cases by County. Johns Hopkins University of Medicine; May 10, 2020. https://coronavirus.jhu.edu/us-map. Accessed April 25, 2020
-
- COVID-19: Data. NYC Health; City of New York: April 24, 2020. https://www1.nyc.gov/site/doh/covid/covid-19-data.page. Accessed April 25, 2020
MeSH terms
LinkOut - more resources
Full Text Sources
Medical